Victor M Neira, Christian D Neira, Kara Matheson, Matthias Scheffler, Renata Morton, Heather E Mingo, Edgar G Chedrawy, Hashem Aliter
{"title":"Rescue Therapy With Factor VII for Refractory Cardiac Surgical Bleeding: A Propensity-Score-Matched Study.","authors":"Victor M Neira, Christian D Neira, Kara Matheson, Matthias Scheffler, Renata Morton, Heather E Mingo, Edgar G Chedrawy, Hashem Aliter","doi":"10.1093/icvts/ivaf185","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To compare effectiveness and safety of rescue therapy approach with recombinant Factor VII activated (rFVIIa) for refractory bleeding in cardiac surgery compared with a propensity-score-matched control group at a single academic institution.</p><p><strong>Methods: </strong>In total, 8860 adult patients had cardiac surgery with cardiopulmonary bypass between 2009 and 2019. Ninety-seven patients (1.1%) received rFVIIa; 81 (83.5%) of rFVIIa cases were propensity score matched 1:1 with controls using pre- and intraoperative variables. Effectiveness was assessed with coagulation tests, chest tube drainage, and reoperation for bleeding. Safety was assessed with morbi-mortality.</p><p><strong>Results: </strong>The median dose of rFVIIa was 55.6 μg/kg (IQR, 37.4-80.0 μg/kg). The first dose after CPB was given at a Median time of 176 min (IQR, 131-232 min). Postoperative INR was lower in the rFVIIa group (Median, 0.8; IQR, 0.7-0.9) versus control (Median, 1.4; IQR 1.3-1.6; P <.0001). Other coagulation tests, chest tube drainage, and reoperation for bleeding were no different. Mortality and thrombo-embolism were higher in the rFVIIa-OR, 3.17 (95% CI, 1.41-7.14; P = .0054) and OR, 10.50 (95% CI, 1.64-117.5; P = .0196). Stroke (OR, 1.82; 95% CI, 0.51-6.48; P = .35) and renal failure (OR, 1.31, 95% CI, 0.69-2.48, P = .41) were not statistically different. RFVIIa group received 4.4 (95% CI, 3.28-5.91, P = .0001) and 1.97 (95% CI, 1.18-3.30; P = .02) times more blood products volume intra- and postoperatively.</p><p><strong>Conclusions: </strong>Rescue therapy with rFVIIa seems to effectively control bleeding. However, we observed an association with increased mortality, thromboembolism, and transfusion. We did not find rFVIIa association with risk of stroke or renal failure.</p>","PeriodicalId":73406,"journal":{"name":"Interdisciplinary cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-08-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12377900/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interdisciplinary cardiovascular and thoracic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/icvts/ivaf185","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To compare effectiveness and safety of rescue therapy approach with recombinant Factor VII activated (rFVIIa) for refractory bleeding in cardiac surgery compared with a propensity-score-matched control group at a single academic institution.
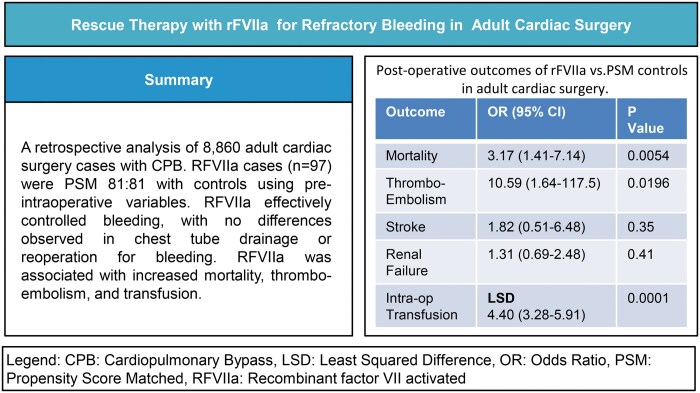
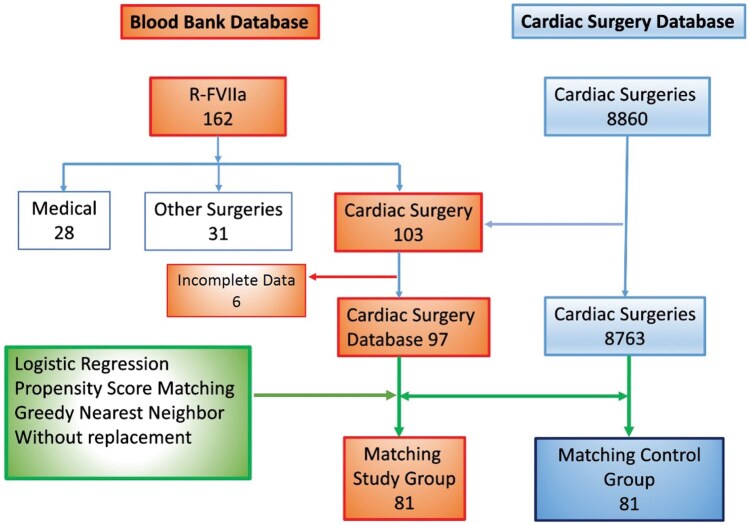
Methods: In total, 8860 adult patients had cardiac surgery with cardiopulmonary bypass between 2009 and 2019. Ninety-seven patients (1.1%) received rFVIIa; 81 (83.5%) of rFVIIa cases were propensity score matched 1:1 with controls using pre- and intraoperative variables. Effectiveness was assessed with coagulation tests, chest tube drainage, and reoperation for bleeding. Safety was assessed with morbi-mortality.
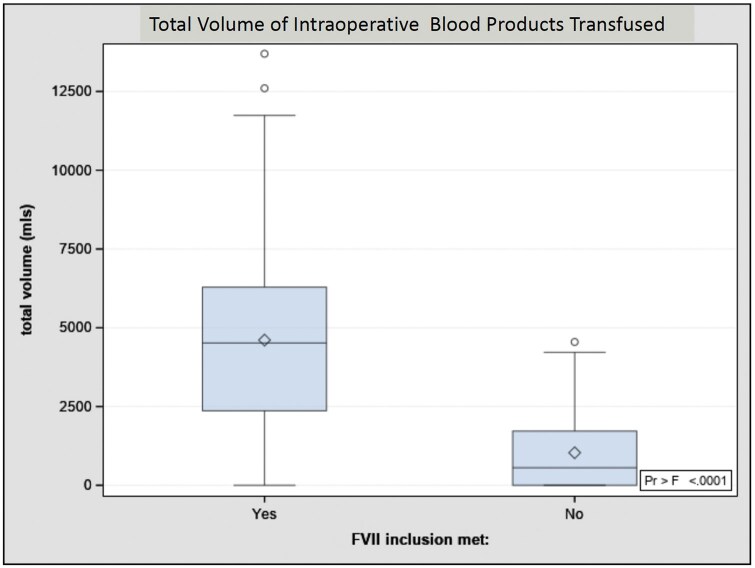
Results: The median dose of rFVIIa was 55.6 μg/kg (IQR, 37.4-80.0 μg/kg). The first dose after CPB was given at a Median time of 176 min (IQR, 131-232 min). Postoperative INR was lower in the rFVIIa group (Median, 0.8; IQR, 0.7-0.9) versus control (Median, 1.4; IQR 1.3-1.6; P <.0001). Other coagulation tests, chest tube drainage, and reoperation for bleeding were no different. Mortality and thrombo-embolism were higher in the rFVIIa-OR, 3.17 (95% CI, 1.41-7.14; P = .0054) and OR, 10.50 (95% CI, 1.64-117.5; P = .0196). Stroke (OR, 1.82; 95% CI, 0.51-6.48; P = .35) and renal failure (OR, 1.31, 95% CI, 0.69-2.48, P = .41) were not statistically different. RFVIIa group received 4.4 (95% CI, 3.28-5.91, P = .0001) and 1.97 (95% CI, 1.18-3.30; P = .02) times more blood products volume intra- and postoperatively.
Conclusions: Rescue therapy with rFVIIa seems to effectively control bleeding. However, we observed an association with increased mortality, thromboembolism, and transfusion. We did not find rFVIIa association with risk of stroke or renal failure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


