Early Atropine Protocol Enhances Dobutamine Stress Echocardiography in End-Stage Liver Disease: A Practical Cardiac Risk Stratification Tool Before Liver Transplantation.
Özge Çetinarslan, Sinan Efe Yazıcı, Ahmet Atasever
{"title":"Early Atropine Protocol Enhances Dobutamine Stress Echocardiography in End-Stage Liver Disease: A Practical Cardiac Risk Stratification Tool Before Liver Transplantation.","authors":"Özge Çetinarslan, Sinan Efe Yazıcı, Ahmet Atasever","doi":"10.12659/AOT.950166","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Chronotropic incompetence often prolongs dobutamine stress echocardiography (DSE) and provokes adverse events in liver-transplant (LT) candidates. We evaluated whether administering atropine 1 stage earlier than conventionally recommended improves test efficiency and tolerability. MATERIAL AND METHODS In this retrospective single-center study, 69 end-stage liver disease patients were assigned to 3 cohorts according to the protocol used: Group 1 - high-dose dobutamine alone (n=24); Group 2 - \"late\" atropine (1 mg at 40 µg/kg/min; n=22); Group 3 - \"early\" atropine (at 30 µg/kg/min; n=23). Primary endpoints were target heart rate (HR) achievement, procedure time, hypotension, and ventricular extrasystole (VES). RESULTS Target HR was reached in 83%, 86%, and 95% of Groups 1-3, respectively (P<0.001). Mean procedure duration fell from 27.82±2.06 min with late atropine to 18.48±0.95 min with early atropine (-33.6%). Hypotension dropped from 50.0% to 8.7% (relative reduction≈83%) and VES decreased from 59.1% to 13.0% (≈78%). Cumulative dobutamine exposure was halved (≈1 113→≈554 µg/kg). No early-atropine patients experienced test-terminating complications. CONCLUSIONS Introducing atropine at the preceding dobutamine stage offers a simple, cost-neutral modification that accelerates DSE, halves drug exposure, and substantially improves hemodynamic and arrhythmic safety in LT candidates. Prospective trials should confirm whether this streamlined protocol can be adopted as the new standard for chronotropically challenging patients.</p>","PeriodicalId":7935,"journal":{"name":"Annals of Transplantation","volume":"30 ","pages":"e950166"},"PeriodicalIF":1.4000,"publicationDate":"2025-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12357517/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Transplantation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.12659/AOT.950166","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
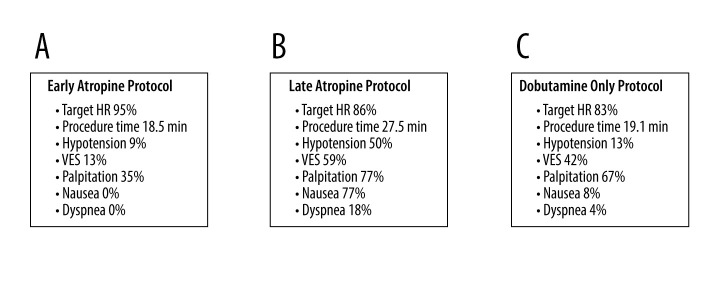
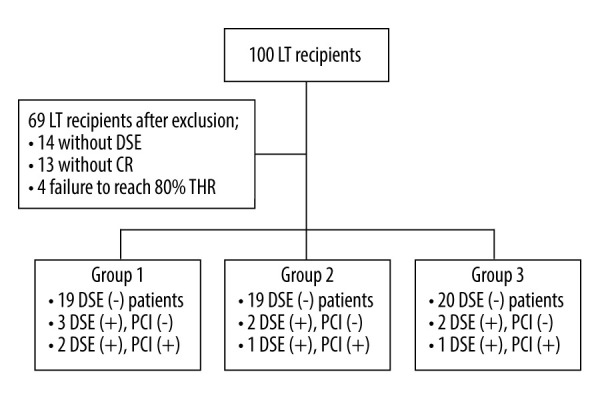
BACKGROUND Chronotropic incompetence often prolongs dobutamine stress echocardiography (DSE) and provokes adverse events in liver-transplant (LT) candidates. We evaluated whether administering atropine 1 stage earlier than conventionally recommended improves test efficiency and tolerability. MATERIAL AND METHODS In this retrospective single-center study, 69 end-stage liver disease patients were assigned to 3 cohorts according to the protocol used: Group 1 - high-dose dobutamine alone (n=24); Group 2 - "late" atropine (1 mg at 40 µg/kg/min; n=22); Group 3 - "early" atropine (at 30 µg/kg/min; n=23). Primary endpoints were target heart rate (HR) achievement, procedure time, hypotension, and ventricular extrasystole (VES). RESULTS Target HR was reached in 83%, 86%, and 95% of Groups 1-3, respectively (P<0.001). Mean procedure duration fell from 27.82±2.06 min with late atropine to 18.48±0.95 min with early atropine (-33.6%). Hypotension dropped from 50.0% to 8.7% (relative reduction≈83%) and VES decreased from 59.1% to 13.0% (≈78%). Cumulative dobutamine exposure was halved (≈1 113→≈554 µg/kg). No early-atropine patients experienced test-terminating complications. CONCLUSIONS Introducing atropine at the preceding dobutamine stage offers a simple, cost-neutral modification that accelerates DSE, halves drug exposure, and substantially improves hemodynamic and arrhythmic safety in LT candidates. Prospective trials should confirm whether this streamlined protocol can be adopted as the new standard for chronotropically challenging patients.
期刊介绍:
Annals of Transplantation is one of the fast-developing journals open to all scientists and fields of transplant medicine and related research. The journal is published quarterly and provides extensive coverage of the most important advances in transplantation.
Using an electronic on-line submission and peer review tracking system, Annals of Transplantation is committed to rapid review and publication. The average time to first decision is around 3-4 weeks. Time to publication of accepted manuscripts continues to be shortened, with the Editorial team committed to a goal of 3 months from acceptance to publication.
Expert reseachers and clinicians from around the world contribute original Articles, Review Papers, Case Reports and Special Reports in every pertinent specialty, providing a lot of arguments for discussion of exciting developments and controversies in the field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


