{"title":"Use of a Pulmonary Artery Catheter in Patients With Cardiogenic Shock - A Systematic Review and Meta-Analysis.","authors":"Toru Kondo, Takahiro Nakashima, Takeshi Yamamoto, Naoki Nakayama, Hiroyuki Hanada, Katsutaka Hashiba, Jin Kirigaya, Tomoko Ishizu, Yumiko Hosoya, Aya Katasako-Yabumoto, Yusuke Okazaki, Masahiro Yamamoto, Kazuo Sakamoto, Marina Arai, Takumi Osawa, Akihito Tanaka, Kunihiro Matsuo, Junichi Yamaguchi, Toshiaki Mano, Sunao Kojima, Teruo Noguchi, Yasushi Tsujimoto, Migaku Kikuchi, Toshikazu Funazaki, Yoshio Tahara, Hiroshi Nonogi, Tetsuya Matoba","doi":"10.1253/circrep.CR-25-0088","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A pulmonary artery catheter (PAC) provides detailed hemodynamic data, and managing a patient with cardiogenic shock (CS) using a PAC potentially improves patient outcomes. Therefore, in this systematic review and meta-analysis we aimed to evaluate whether a PAC is associated with better outcomes in patients with CS.</p><p><strong>Methods and results: </strong>Studies comparing PAC and non-PAC management in patients with CS were identified from the PubMed, Web of Science, and CENTRAL databases. There were no randomized controlled trials (RCTs). Of the 19 studies that met the inclusion criteria, 12 without a critical risk of bias were analyzed. PAC use was associated with lower in-hospital mortality when evaluated as a dichotomous outcome. Similar trends were observed in the time-to-event analyses. Substantial heterogeneity was observed across the studies. Subgroup analysis revealed better outcomes with PAC in patients with CS related to heart failure, but not in those with acute coronary syndrome. Sensitivity analyses, which included studies with a critical risk of bias, showed consistent trends favoring PAC use for crude in-hospital mortality. The overall certainty of the evidence was very low because of inconsistencies and biases.</p><p><strong>Conclusions: </strong>The PAC-guided CS management was associated with better in-hospital mortality, particularly in patients with heart failure-related CS. However, RCTs that evaluated the efficacy of PAC use as a primary purpose were not included, necessitating further RCTs to confirm these findings.</p>","PeriodicalId":94305,"journal":{"name":"Circulation reports","volume":"7 8","pages":"589-598"},"PeriodicalIF":1.1000,"publicationDate":"2025-07-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331356/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-25-0088","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/8 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A pulmonary artery catheter (PAC) provides detailed hemodynamic data, and managing a patient with cardiogenic shock (CS) using a PAC potentially improves patient outcomes. Therefore, in this systematic review and meta-analysis we aimed to evaluate whether a PAC is associated with better outcomes in patients with CS.
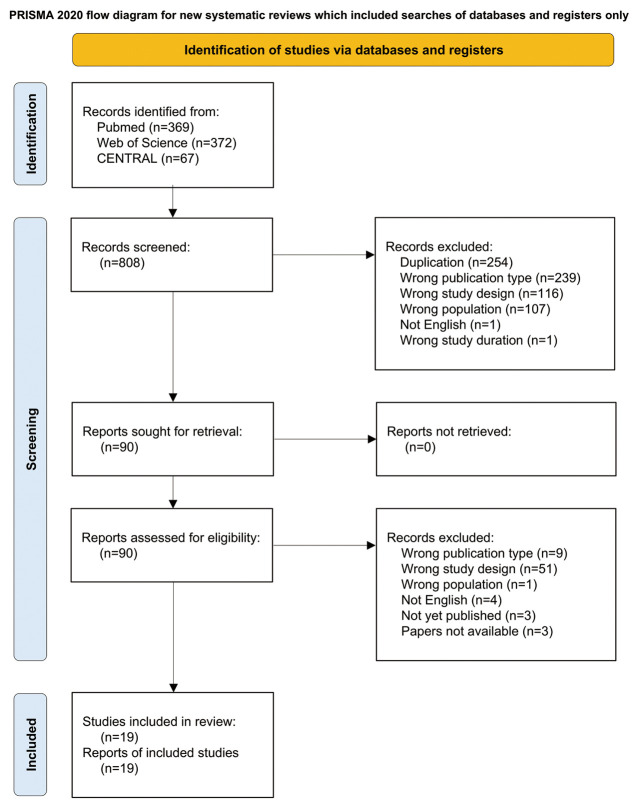
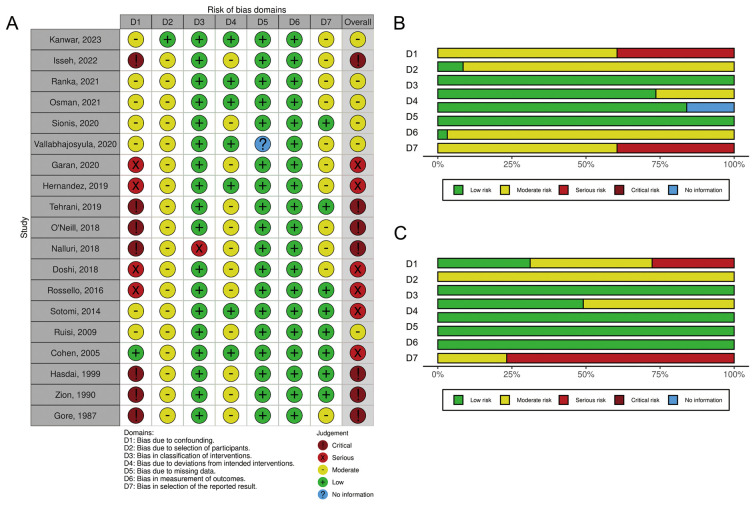
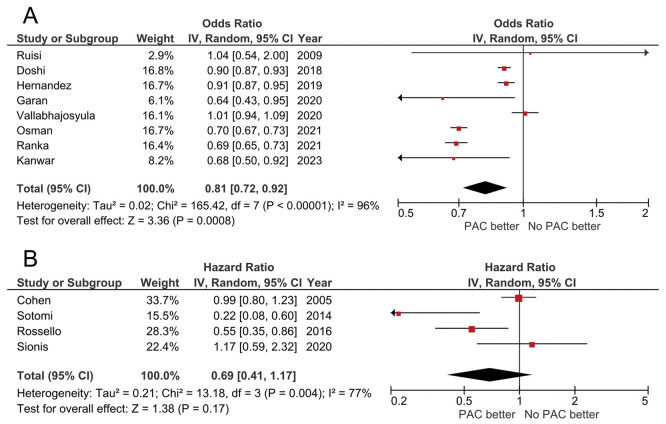
Methods and results: Studies comparing PAC and non-PAC management in patients with CS were identified from the PubMed, Web of Science, and CENTRAL databases. There were no randomized controlled trials (RCTs). Of the 19 studies that met the inclusion criteria, 12 without a critical risk of bias were analyzed. PAC use was associated with lower in-hospital mortality when evaluated as a dichotomous outcome. Similar trends were observed in the time-to-event analyses. Substantial heterogeneity was observed across the studies. Subgroup analysis revealed better outcomes with PAC in patients with CS related to heart failure, but not in those with acute coronary syndrome. Sensitivity analyses, which included studies with a critical risk of bias, showed consistent trends favoring PAC use for crude in-hospital mortality. The overall certainty of the evidence was very low because of inconsistencies and biases.
Conclusions: The PAC-guided CS management was associated with better in-hospital mortality, particularly in patients with heart failure-related CS. However, RCTs that evaluated the efficacy of PAC use as a primary purpose were not included, necessitating further RCTs to confirm these findings.
背景:肺动脉导管(PAC)提供详细的血流动力学数据,使用PAC处理心源性休克(CS)患者可能会改善患者的预后。因此,在本系统综述和荟萃分析中,我们旨在评估PAC是否与CS患者更好的预后相关。方法和结果:从PubMed、Web of Science和CENTRAL数据库中确定了比较CS患者PAC和非PAC管理的研究。没有随机对照试验(rct)。在符合纳入标准的19项研究中,分析了12项没有严重偏倚风险的研究。当作为二分类结果评估时,PAC的使用与较低的住院死亡率相关。在事件时间分析中也观察到类似的趋势。在研究中观察到大量的异质性。亚组分析显示,PAC治疗与心力衰竭相关的CS患者预后较好,而急性冠状动脉综合征患者预后较差。敏感性分析,包括具有严重偏倚风险的研究,显示了一贯倾向于使用PAC来降低住院死亡率的趋势。由于不一致和偏见,证据的总体确定性非常低。结论:pac引导的CS管理与更好的住院死亡率相关,特别是心力衰竭相关的CS患者。然而,评估PAC使用作为主要目的的疗效的随机对照试验并未纳入,因此需要进一步的随机对照试验来证实这些发现。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


