Comparison of Short-Term Clinical Outcomes Between Intravascular Lithotripsy and Rotational Atherectomy for Calcified Coronary Stenosis in Patients With Acute Coronary Syndrome.
{"title":"Comparison of Short-Term Clinical Outcomes Between Intravascular Lithotripsy and Rotational Atherectomy for Calcified Coronary Stenosis in Patients With Acute Coronary Syndrome.","authors":"Yasuhiro Honda, Kensaku Nishihira, Nehiro Kuriyama, Makoto Takamatsu, Keisuke Yamamoto, Shun Nishino, Kosuke Kadooka, Takeaki Kudo, Kenji Ogata, Toshiyuki Kimura, Kengo Ayabe, Keiichi Ashikaga, Yoshisato Shibata","doi":"10.1253/circrep.CR-25-0086","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The optimal revascularization strategy for calcified lesions in patients with acute coronary syndrome (ACS) remains unclear. This study aimed to compare the short-term outcomes of intravascular lithotripsy (IVL) and rotational atherectomy (RA) for patients with ACS resulting from calcified lesions.</p><p><strong>Methods and results: </strong>Among 3,556 consecutive patients with ACS who underwent primary percutaneous coronary intervention (PCI) between 2016 and 2024, we retrospectively analyzed 52 patients who received drug-eluting stents with either IVL (n=24) or RA (n=28) for calcified lesions. The primary outcome was the incidence of major adverse cardiovascular events (MACE). In addition, we evaluated slow-flow or no-reflow phenomena incidence during PCI and the procedural success rate. Compared with patients with RA, those with IVL had a smaller preprocedural minimum lumen diameter and a larger preprocedural reference vessel diameter. Primary outcomes and procedural success rates were comparable between both groups. However, the slow-flow or no-reflow incidence was significantly lower in the IVL group than in the RA group. After adjusting for confounders, IVL was independently associated with a lower slow-flow or no-reflow incidence.</p><p><strong>Conclusions: </strong>In patients with ACS due to calcified lesions, there was no significant difference in 30-day MACE incidence between both groups. However, slow-flow incidence was lower in the IVL group.</p>","PeriodicalId":94305,"journal":{"name":"Circulation reports","volume":"7 8","pages":"612-618"},"PeriodicalIF":1.1000,"publicationDate":"2025-07-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331347/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-25-0086","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/8 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The optimal revascularization strategy for calcified lesions in patients with acute coronary syndrome (ACS) remains unclear. This study aimed to compare the short-term outcomes of intravascular lithotripsy (IVL) and rotational atherectomy (RA) for patients with ACS resulting from calcified lesions.
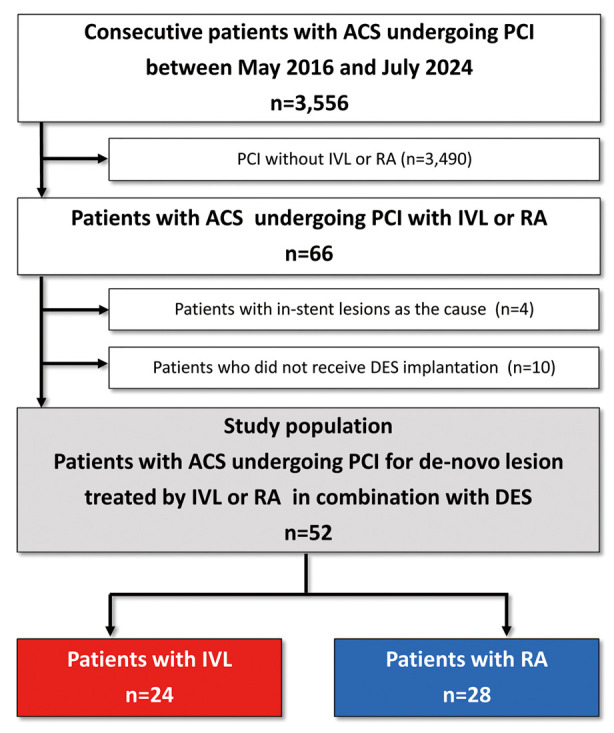
Methods and results: Among 3,556 consecutive patients with ACS who underwent primary percutaneous coronary intervention (PCI) between 2016 and 2024, we retrospectively analyzed 52 patients who received drug-eluting stents with either IVL (n=24) or RA (n=28) for calcified lesions. The primary outcome was the incidence of major adverse cardiovascular events (MACE). In addition, we evaluated slow-flow or no-reflow phenomena incidence during PCI and the procedural success rate. Compared with patients with RA, those with IVL had a smaller preprocedural minimum lumen diameter and a larger preprocedural reference vessel diameter. Primary outcomes and procedural success rates were comparable between both groups. However, the slow-flow or no-reflow incidence was significantly lower in the IVL group than in the RA group. After adjusting for confounders, IVL was independently associated with a lower slow-flow or no-reflow incidence.
Conclusions: In patients with ACS due to calcified lesions, there was no significant difference in 30-day MACE incidence between both groups. However, slow-flow incidence was lower in the IVL group.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


