{"title":"Lymphedema and Axillary-Lateral Thoracic Vessel Juncture Irradiation: A Clinical Dilemma.","authors":"Şükran Şenyürek, Merve Duman, Sena Birsen Güçlü, Nilüfer Kılıç Durankuş, Duygu Sezen, Yasemin Bölükbaşı","doi":"10.4274/ejbh.galenos.2025.2025-2-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Regional nodal irradiation (RNI) is one of the main causes of breast cancer-related lymphedema (BCRL). However, studies on the relationship between the radiation dose to the axillary-lateral thoracic vessel juncture (ALTJ) region and BCRL have reported conflicting results. Based on these findings, we aimed to evaluate the clinical relevance of the dose to the ALTJ region in our patient cohort.</p><p><strong>Materials and methods: </strong>Patients diagnosed with breast cancer and who were treated at Koç University Hospital between 2016 and 2022 and received RNI were included. BCRL was defined as a difference in arm circumference between the ipsilateral and contralateral limb >2.5 cm at any single encounter or ≥2 cm on ≥2 visits. ALTJ was retrospectively contoured, and doses were recorded as equivalent dose (α/β = 3).</p><p><strong>Results: </strong>Of the 129 patients (median age 49 years) who met the inclusion criteria, 12 (9.3%) had lymphedema. Two-thirds of the patients (66.7%) were stage II, and one-third (33.3%) were stage III. The median follow-up was 22 months. The median (range) ALTJ D<sub>mean</sub> dose was 18.11 (1.87-50) Gy, the median ALTJ D<sub>max</sub> was 44.53 (12.8-71.1) Gy, and the median ALTJ V35 was 38% (1-100%). No significant association was determined between ALTJ parameters and BCRL.</p><p><strong>Conclusion: </strong>There is insufficient data to define ALTJ as an OAR for decreasing BCRL risk. It is not appropriate to define dose and target based on ALTJ. Prospective studies with larger patient populations are needed to clarify the relationship between ALTJ and lymphedema.</p>","PeriodicalId":93996,"journal":{"name":"European journal of breast health","volume":" ","pages":"301-306"},"PeriodicalIF":1.7000,"publicationDate":"2025-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12462729/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of breast health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4274/ejbh.galenos.2025.2025-2-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/4 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Regional nodal irradiation (RNI) is one of the main causes of breast cancer-related lymphedema (BCRL). However, studies on the relationship between the radiation dose to the axillary-lateral thoracic vessel juncture (ALTJ) region and BCRL have reported conflicting results. Based on these findings, we aimed to evaluate the clinical relevance of the dose to the ALTJ region in our patient cohort.
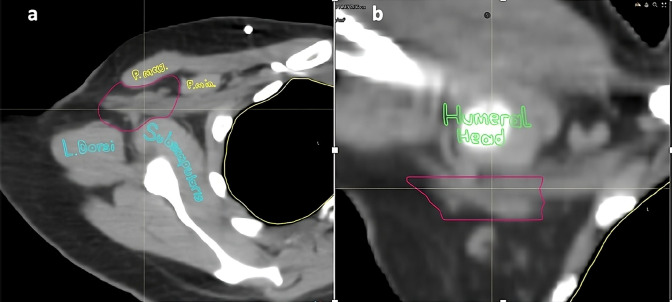
Materials and methods: Patients diagnosed with breast cancer and who were treated at Koç University Hospital between 2016 and 2022 and received RNI were included. BCRL was defined as a difference in arm circumference between the ipsilateral and contralateral limb >2.5 cm at any single encounter or ≥2 cm on ≥2 visits. ALTJ was retrospectively contoured, and doses were recorded as equivalent dose (α/β = 3).
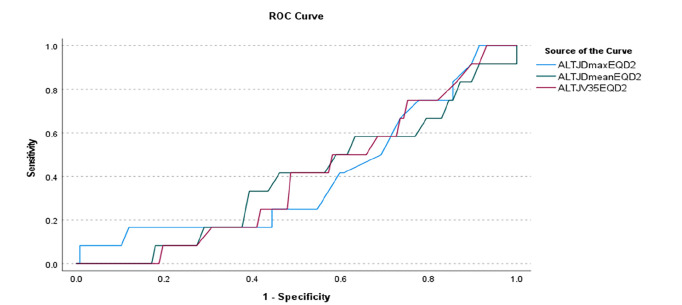
Results: Of the 129 patients (median age 49 years) who met the inclusion criteria, 12 (9.3%) had lymphedema. Two-thirds of the patients (66.7%) were stage II, and one-third (33.3%) were stage III. The median follow-up was 22 months. The median (range) ALTJ Dmean dose was 18.11 (1.87-50) Gy, the median ALTJ Dmax was 44.53 (12.8-71.1) Gy, and the median ALTJ V35 was 38% (1-100%). No significant association was determined between ALTJ parameters and BCRL.
Conclusion: There is insufficient data to define ALTJ as an OAR for decreasing BCRL risk. It is not appropriate to define dose and target based on ALTJ. Prospective studies with larger patient populations are needed to clarify the relationship between ALTJ and lymphedema.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


