Shinichi Togami, Nozomi Furuzono, Mika Fukuda, Hiroaki Kobayashi
{"title":"Comparative Long-term Outcomes of Laparoscopic Radical Hysterectomy with Sentinel Node Navigation and Open Surgery for Cervical Cancer.","authors":"Shinichi Togami, Nozomi Furuzono, Mika Fukuda, Hiroaki Kobayashi","doi":"10.4103/gmit.GMIT-D-24-00003","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Minimally invasive surgery (MIS) for cervical cancer is associated with poorer outcomes compared with open surgery. The Laparoscopic Approach to Cervical Cancer trial revealed an increased recurrence and mortality risk after MIS. We aimed to compare the long-term outcomes of laparoscopic radical hysterectomy (LRH) with those of sentinel node navigation surgery (SNNS) and open surgery for cervical cancer, emphasizing techniques to prevent cancer spillages.</p><p><strong>Materials and methods: </strong>We retrospectively analyzed data from 103 patients with cervical cancer who underwent radical hysterectomy at Kagoshima University Hospital between 2007 and 2023. The patients were divided into the LRH with SNNS and open surgery groups. All LRH procedures involved closing the vagina using a vaginal cuff without a uterine manipulator. Clinicopathological factors and oncological outcomes, including 5-year recurrence-free survival (RFS) and overall survival (OS), were compared between the groups.</p><p><strong>Results: </strong>The 5-year RFS and OS rates were 92.7% and 94% and 85.5% and 88.3% for LRH and open surgery, respectively, with no significant intergroup differences. No peritoneal dissemination or recurrence was observed in the LRH group. LRH with SNNS procedure achieved 100% sentinel node identification, and lower extremity lymphedema or pelvic lymphocele did not occur.</p><p><strong>Conclusion: </strong>LRH with SNNS and open surgery for cervical cancer exhibited comparable long-term outcomes. Vaginal closure using a vaginal cuff without a uterine manipulator is crucial for preventing cancer spillage. Combining LRH with SNNS is less invasive and avoids compromising oncological outcomes. High-quality randomized controlled trials are required to validate these findings.</p>","PeriodicalId":45272,"journal":{"name":"Gynecology and Minimally Invasive Therapy-GMIT","volume":"14 3","pages":"234-240"},"PeriodicalIF":1.7000,"publicationDate":"2025-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12334094/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gynecology and Minimally Invasive Therapy-GMIT","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/gmit.GMIT-D-24-00003","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Minimally invasive surgery (MIS) for cervical cancer is associated with poorer outcomes compared with open surgery. The Laparoscopic Approach to Cervical Cancer trial revealed an increased recurrence and mortality risk after MIS. We aimed to compare the long-term outcomes of laparoscopic radical hysterectomy (LRH) with those of sentinel node navigation surgery (SNNS) and open surgery for cervical cancer, emphasizing techniques to prevent cancer spillages.
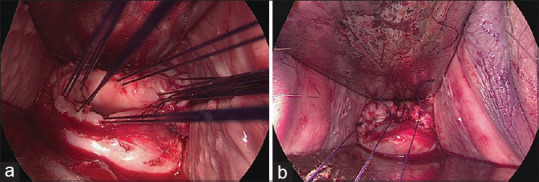
Materials and methods: We retrospectively analyzed data from 103 patients with cervical cancer who underwent radical hysterectomy at Kagoshima University Hospital between 2007 and 2023. The patients were divided into the LRH with SNNS and open surgery groups. All LRH procedures involved closing the vagina using a vaginal cuff without a uterine manipulator. Clinicopathological factors and oncological outcomes, including 5-year recurrence-free survival (RFS) and overall survival (OS), were compared between the groups.
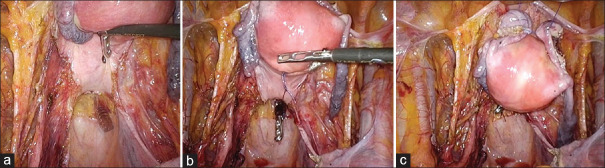
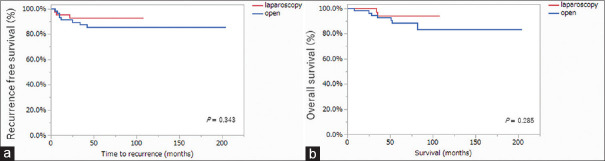
Results: The 5-year RFS and OS rates were 92.7% and 94% and 85.5% and 88.3% for LRH and open surgery, respectively, with no significant intergroup differences. No peritoneal dissemination or recurrence was observed in the LRH group. LRH with SNNS procedure achieved 100% sentinel node identification, and lower extremity lymphedema or pelvic lymphocele did not occur.
Conclusion: LRH with SNNS and open surgery for cervical cancer exhibited comparable long-term outcomes. Vaginal closure using a vaginal cuff without a uterine manipulator is crucial for preventing cancer spillage. Combining LRH with SNNS is less invasive and avoids compromising oncological outcomes. High-quality randomized controlled trials are required to validate these findings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


