Safety and Efficacy of Fecal Microbiota, Live-jslm to Prevent Recurrent Clostridioides difficile Infection in Participants With Irritable Bowel Syndrome.
Olga C Aroniadis, Beth Guthmueller, Kaitlin Dehlin, Shivam Srivastava, Paul Feuerstadt, Anthony Lembo, Horst C Weber
{"title":"Safety and Efficacy of Fecal Microbiota, Live-jslm to Prevent Recurrent Clostridioides difficile Infection in Participants With Irritable Bowel Syndrome.","authors":"Olga C Aroniadis, Beth Guthmueller, Kaitlin Dehlin, Shivam Srivastava, Paul Feuerstadt, Anthony Lembo, Horst C Weber","doi":"10.1007/s40121-025-01208-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The safety and efficacy of microbiota-based products in patients with irritable bowel syndrome (IBS) and recurrent Clostridioides difficile infection (rCDI) has not been studied. Fecal microbiota, live-jslm (RBL; REBYOTA<sup>®</sup>) is an FDA-approved, single-dose, microbiota-based product to prevent rCDI in adults following standard-of-care (SOC) antibiotic treatment. This was an exploratory subgroup analysis of PUNCH CD3-OLS, a phase 3, open-label, prospective study conducted in the United States (US) and Canada, to evaluate the safety and efficacy of RBL in participants with documented rCDI and concurrent IBS.</p><p><strong>Methods: </strong>Participants aged ≥ 18 years with a diagnosis of rCDI and who completed SOC antibiotic treatment were enrolled in this study. The primary endpoint of PUNCH CD3-OLS was the number of participants with RBL- or administration-related treatment-emergent adverse events (TEAEs). Secondary endpoints included treatment success at 8 weeks and sustained clinical response at 6 months. In this subgroup analysis, ongoing IBS was confirmed based on medical record documentation at the time of RBL administration.</p><p><strong>Results: </strong>Among the 697 RBL recipients, 90 had comorbid IBS. After RBL administration, 52 participants with IBS (57.8%) and 278 participants without IBS (45.8%) experienced TEAEs through 8 weeks. Most TEAEs were mild (22.2% with IBS, 20.1% without IBS) or moderate (26.7% with IBS, 18.8% without IBS). Serious TEAEs were reported by 1 participant with IBS (pneumonia reported to be unrelated to RBL) and 26 participants without IBS [most of which were related to preexisting conditions (3.1%)]. Among all participants, 68.9% with IBS and 75.6% without IBS had absence of CDI diarrhea through 8 weeks after RBL administration. Of the participants with treatment success, 82.3% with IBS and 92.2% without IBS had sustained clinical response through 6 months.</p><p><strong>Conclusion: </strong>RBL is a safe and efficacious option to prevent CDI recurrence in patients with concurrent IBS.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov identifier, NCT03931941.</p>","PeriodicalId":13592,"journal":{"name":"Infectious Diseases and Therapy","volume":" ","pages":"2157-2169"},"PeriodicalIF":5.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12425869/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Diseases and Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40121-025-01208-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/10 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The safety and efficacy of microbiota-based products in patients with irritable bowel syndrome (IBS) and recurrent Clostridioides difficile infection (rCDI) has not been studied. Fecal microbiota, live-jslm (RBL; REBYOTA®) is an FDA-approved, single-dose, microbiota-based product to prevent rCDI in adults following standard-of-care (SOC) antibiotic treatment. This was an exploratory subgroup analysis of PUNCH CD3-OLS, a phase 3, open-label, prospective study conducted in the United States (US) and Canada, to evaluate the safety and efficacy of RBL in participants with documented rCDI and concurrent IBS.
Methods: Participants aged ≥ 18 years with a diagnosis of rCDI and who completed SOC antibiotic treatment were enrolled in this study. The primary endpoint of PUNCH CD3-OLS was the number of participants with RBL- or administration-related treatment-emergent adverse events (TEAEs). Secondary endpoints included treatment success at 8 weeks and sustained clinical response at 6 months. In this subgroup analysis, ongoing IBS was confirmed based on medical record documentation at the time of RBL administration.
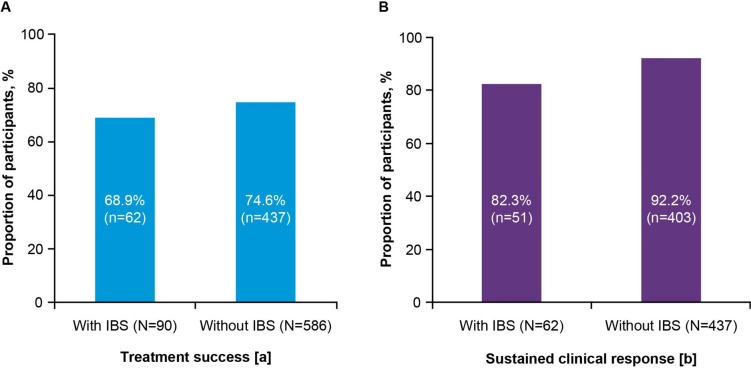
Results: Among the 697 RBL recipients, 90 had comorbid IBS. After RBL administration, 52 participants with IBS (57.8%) and 278 participants without IBS (45.8%) experienced TEAEs through 8 weeks. Most TEAEs were mild (22.2% with IBS, 20.1% without IBS) or moderate (26.7% with IBS, 18.8% without IBS). Serious TEAEs were reported by 1 participant with IBS (pneumonia reported to be unrelated to RBL) and 26 participants without IBS [most of which were related to preexisting conditions (3.1%)]. Among all participants, 68.9% with IBS and 75.6% without IBS had absence of CDI diarrhea through 8 weeks after RBL administration. Of the participants with treatment success, 82.3% with IBS and 92.2% without IBS had sustained clinical response through 6 months.
Conclusion: RBL is a safe and efficacious option to prevent CDI recurrence in patients with concurrent IBS.
期刊介绍:
Infectious Diseases and Therapy is an international, open access, peer-reviewed, rapid publication journal dedicated to the publication of high-quality clinical (all phases), observational, real-world, and health outcomes research around the discovery, development, and use of infectious disease therapies and interventions, including vaccines and devices. Studies relating to diagnostic products and diagnosis, pharmacoeconomics, public health, epidemiology, quality of life, and patient care, management, and education are also encouraged.
Areas of focus include, but are not limited to, bacterial and fungal infections, viral infections (including HIV/AIDS and hepatitis), parasitological diseases, tuberculosis and other mycobacterial diseases, vaccinations and other interventions, and drug-resistance, chronic infections, epidemiology and tropical, emergent, pediatric, dermal and sexually-transmitted diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


