Allahdad Khan, Abdul Ahad Riaz, Shahroze Ahmed, Anam Malik, Mohamed Antar, Raheel Ahmed
{"title":"Solitary brain metastasis from laryngeal squamous cell carcinoma in a 68-year-old male: A Case Report.","authors":"Allahdad Khan, Abdul Ahad Riaz, Shahroze Ahmed, Anam Malik, Mohamed Antar, Raheel Ahmed","doi":"10.1097/MS9.0000000000003549","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction and importance: </strong>Laryngeal squamous cell carcinoma (LSCC) commonly metastasizes to regional lymph nodes, lungs, liver, and bones. Intracranial metastasis from LSCC is exceedingly rare, reported in only 0.4% of cases. The atypical presentation can delay diagnosis and negatively impact prognosis. We report a rare case of solitary brain metastasis from LSCC, highlighting the diagnostic challenges and clinical considerations.</p><p><strong>Case presentation: </strong>A 68-year-old Pakistani male with a prior diagnosis of LSCC presented with new-onset generalized tonic-clonic seizures. He had previously undergone total laryngectomy, radiotherapy, and chemotherapy. Brain MRI revealed a right frontal lobe lesion with surrounding edema, consistent with a solitary metastasis. Histopathology following craniotomy confirmed metastatic squamous cell carcinoma. The patient was managed with antiepileptics and referred for palliative whole-brain radiotherapy. He and his family opted for palliative care, declining further aggressive treatment.</p><p><strong>Clinical discussion: </strong>Distant brain metastasis in LSCC is rare and may occur without prior systemic spread. The mechanism may involve perineural invasion, although the exact pathophysiology remains unclear. Current diagnostic approaches include MRI and FDG-PET/CT. Due to limited cases, standardized treatment protocols are lacking. Management options include surgery, radiotherapy, chemotherapy, and palliative care, depending on disease progression and patient preference. Seizures as a presenting symptom are uncommon but may indicate intracranial involvement.</p><p><strong>Conclusion: </strong>This case emphasizes the need for high clinical suspicion and comprehensive neurological assessment in patients with advanced LSCC. Early diagnosis and multidisciplinary management are essential for improving outcomes in this rare but serious manifestation.</p>","PeriodicalId":8025,"journal":{"name":"Annals of Medicine and Surgery","volume":"87 8","pages":"5296-5299"},"PeriodicalIF":1.6000,"publicationDate":"2025-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12333697/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Medicine and Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/MS9.0000000000003549","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction and importance: Laryngeal squamous cell carcinoma (LSCC) commonly metastasizes to regional lymph nodes, lungs, liver, and bones. Intracranial metastasis from LSCC is exceedingly rare, reported in only 0.4% of cases. The atypical presentation can delay diagnosis and negatively impact prognosis. We report a rare case of solitary brain metastasis from LSCC, highlighting the diagnostic challenges and clinical considerations.
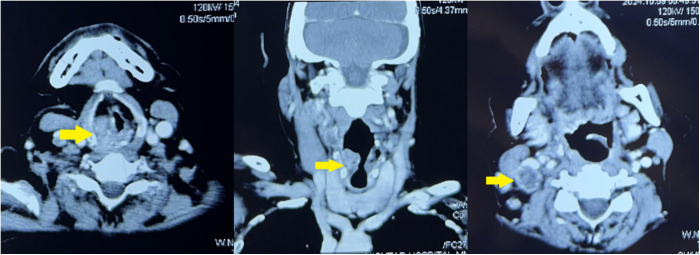
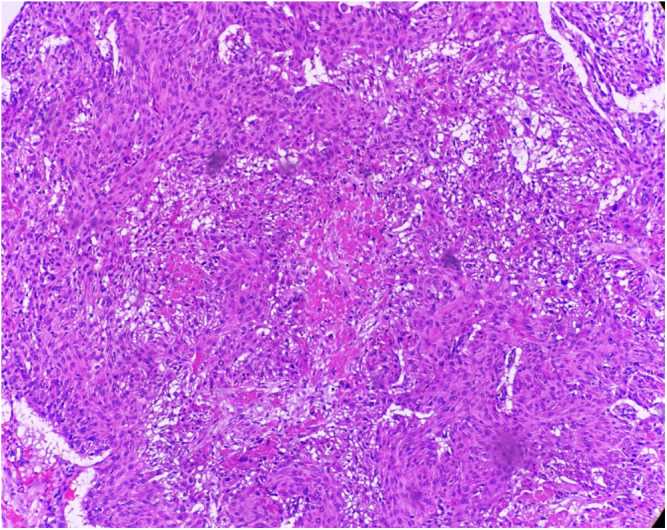
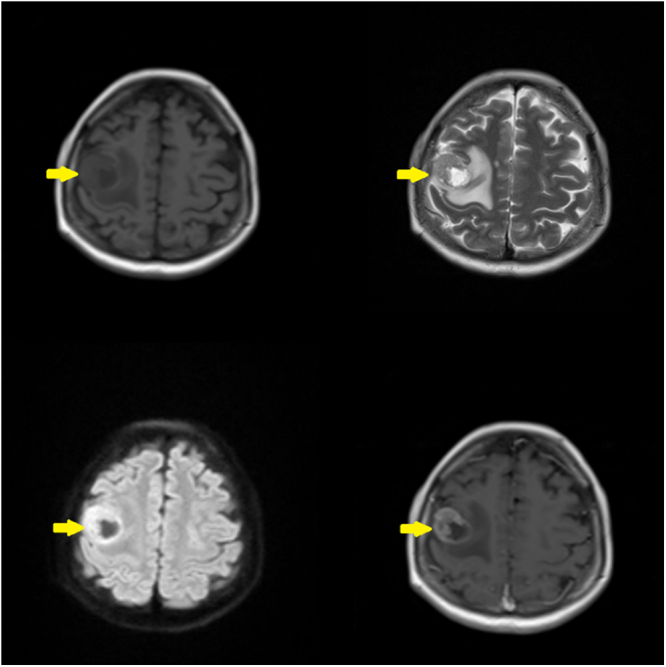
Case presentation: A 68-year-old Pakistani male with a prior diagnosis of LSCC presented with new-onset generalized tonic-clonic seizures. He had previously undergone total laryngectomy, radiotherapy, and chemotherapy. Brain MRI revealed a right frontal lobe lesion with surrounding edema, consistent with a solitary metastasis. Histopathology following craniotomy confirmed metastatic squamous cell carcinoma. The patient was managed with antiepileptics and referred for palliative whole-brain radiotherapy. He and his family opted for palliative care, declining further aggressive treatment.
Clinical discussion: Distant brain metastasis in LSCC is rare and may occur without prior systemic spread. The mechanism may involve perineural invasion, although the exact pathophysiology remains unclear. Current diagnostic approaches include MRI and FDG-PET/CT. Due to limited cases, standardized treatment protocols are lacking. Management options include surgery, radiotherapy, chemotherapy, and palliative care, depending on disease progression and patient preference. Seizures as a presenting symptom are uncommon but may indicate intracranial involvement.
Conclusion: This case emphasizes the need for high clinical suspicion and comprehensive neurological assessment in patients with advanced LSCC. Early diagnosis and multidisciplinary management are essential for improving outcomes in this rare but serious manifestation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


