Beyond STEMI: High-risk ECG patterns as predictors of occlusive myocardial infarction in out-of-hospital cardiac arrest patients
IF 4.6
1区 医学
Q1 CRITICAL CARE MEDICINE
引用次数: 0
Abstract
Background/Aim
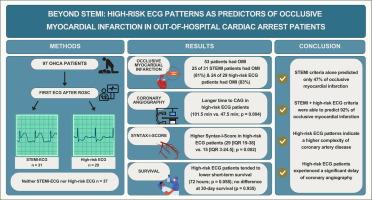
Immediate coronary angiography (CAG) is recommended for patients with ST-elevation myocardial infarction (STEMI) after out-of-hospital cardiac arrest (OHCA). However, some occlusive myocardial infarctions (OMI) do not meet STEMI criteria. This study investigated whether additional ECG patterns beyond STEMI could more accurately identify OMI in OHCA patients, compared to using STEMI criteria alone.
Methods
This retrospective study categorised patients based on their first post-resuscitation ECG into two groups: STEMI and non-STEMI with high-risk ECG criteria and compared them for OMI by CAG.
Results
Among 97 patients OMI was identified in 55 % (53/97) of patients, specifically in 25 of 31 with STEMI (81 %), 24 of 29 with high-risk ECG (83 %), and 4 of 37 patients with neither (11 %). Combining STEMI and high-risk ECG criteria would have predicted OMI in 92 % (49/53) of cases. Patients with high-risk ECG experienced significantly longer median delays until CAG (101.5 [IQR 63–336.75] vs. 47.5 [25.75–71.25] minutes; p = 0.004) compared to those with STEMI on the ECG. Although 30-day mortality did not differ between STEMI and high-risk ECG patients (p = 0.973), survival-differences could be observed between groups. Syntax-I-Score was significantly higher in the high-risk ECG group (29 [IQR 19–38] vs. 15 [IQR 3–24.5]; p = 0.002).
Conclusion
Combining STEMI and high-risk ECG criteria improves OMI prediction compared to STEMI criteria alone, potentially enabling faster treatment and better OHCA survival.
超越STEMI:院外心脏骤停患者的高危心电图模式作为闭塞性心肌梗死的预测因素。
背景/目的:院外心脏骤停(OHCA)后st段抬高型心肌梗死(STEMI)患者推荐立即冠状动脉造影(CAG)。然而,一些闭塞性心肌梗死(OMI)不符合STEMI标准。本研究调查了与单独使用STEMI标准相比,STEMI之外的其他心电图模式是否能更准确地识别OHCA患者的OMI。方法:本回顾性研究根据复苏后首次心电图将患者分为两组:STEMI和非STEMI高危心电图标准,并通过CAG比较他们的OMI。结果:在97例患者中,55%(53/97)的患者发现了OMI,其中31例STEMI患者中有25例(81%),29例高危心电图患者中有24例(83%),37例无高危心电图患者中有4例(11%)。结合STEMI和高危心电图标准可以预测92%(49/53)的病例发生OMI。高危心电图患者延迟到CAG的中位时间明显更长(101.5 [IQR 63 - 336.75] vs. 47.5[25.75 - 71.25]分钟;p = 0.004)与STEMI高危心电图患者相比,STEMI患者30天死亡率无显著差异(p = 0.973),但两组间存在生存差异。高危心电图组Syntax-I-Score显著增高(29 [IQR 19 - 38] vs. 15 [IQR 3 - 24.5];P = 0.002)。结论:与单独STEMI标准相比,STEMI和高危心电图标准联合可改善OMI预测,可能使治疗更快,OHCA生存率更高。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Resuscitation
医学-急救医学
CiteScore
12.00
自引率
18.50%
发文量
556
审稿时长
21 days
期刊介绍:
Resuscitation is a monthly international and interdisciplinary medical journal. The papers published deal with the aetiology, pathophysiology and prevention of cardiac arrest, resuscitation training, clinical resuscitation, and experimental resuscitation research, although papers relating to animal studies will be published only if they are of exceptional interest and related directly to clinical cardiopulmonary resuscitation. Papers relating to trauma are published occasionally but the majority of these concern traumatic cardiac arrest.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


