{"title":"Corneal neurotization meets COVID-19: a case report of minimally invasive corneal neurotization complicated by COVID-19-related keratitis.","authors":"Shuqin Zhuang, Qiaoran Qi, Jiaying Zhang, Jin Li","doi":"10.1186/s12348-025-00521-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To report a rare case of severe keratitis followed by SARS-CoV-2 infection after minimally invasive corneal neurotization (MICN) surgery for the first time.</p><p><strong>Methods: </strong>Retrospective single case report.</p><p><strong>Results: </strong>A 59-year-old female presented to ophthalmology department of our hospital with facial paralysis induced by neurosurgeries. After detailed ophthalmological examination, she was diagnosed with Mackie stage III neurotrophic keratopathy (NK) in the right eye and subsequently underwent MICN and amniotic membrane transplantation. Postoperatively, corneal sensation and the epithelial defect showed gradual improvement, with corneal sensation recovering to 30 mm (measured by Cochet-Bonnet esthesiometer). However, thirteen months after MICN, she developed a corneal ulcer in the right eye one week after contracting SARS-CoV-2 (COVID-19). Supplementary investigations, including anterior segment photography, in vivo confocal microscopy (IVCM), and corneal scraping for pathogen detection, revealed recurrent corneal anesthesia and loss of corneal nerves, with no pathogens identified. After two weeks of empirical antiviral and antibacterial therapy yielded no significant improvement, a diagnosis of COVID-19-induced neurotrophic keratitis (Stage III Mackie) was established. Management consisted of prolonged medical therapy (including antiviral agents, antibiotics, nutritional supplementation, corticosteroids, and artificial tears), two amniotic membrane transplants, and one temporary tarsorrhaphy. Following two years of treatment and follow-up, the corneal lesion achieved complete healing with corneal nerve regeneration and restoration of corneal sensation.</p><p><strong>Conclusion: </strong>This study presents the first documented case of COVID-19-related NK following MICN established as a diagnosis of exclusion. This case underscores the critical need for comprehensive differential diagnosis to rule out infectious etiologies in post-MICN keratitis, ultimately leading to a diagnosis of exclusion for COVID-19-induced disease. The diagnostic approach outlined may offer valuable insights for similar presentations. After a protracted clinical course, the patient ultimately achieved restoration of corneal sensation and reinnervation, demonstrating the preserved regenerative potential of MICN-reconstructed neural pathways even after severe viral infection.</p>","PeriodicalId":16600,"journal":{"name":"Journal of Ophthalmic Inflammation and Infection","volume":"15 1","pages":"60"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12335426/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Ophthalmic Inflammation and Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12348-025-00521-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To report a rare case of severe keratitis followed by SARS-CoV-2 infection after minimally invasive corneal neurotization (MICN) surgery for the first time.
Methods: Retrospective single case report.
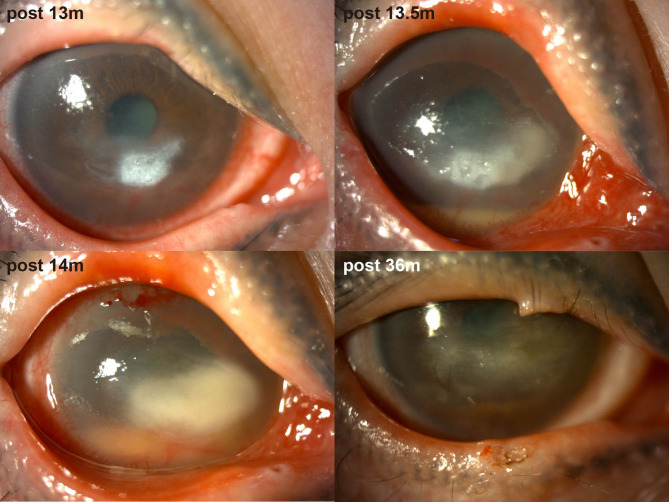
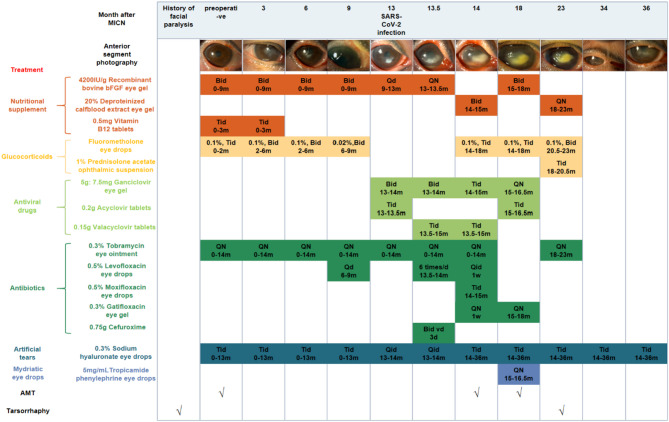
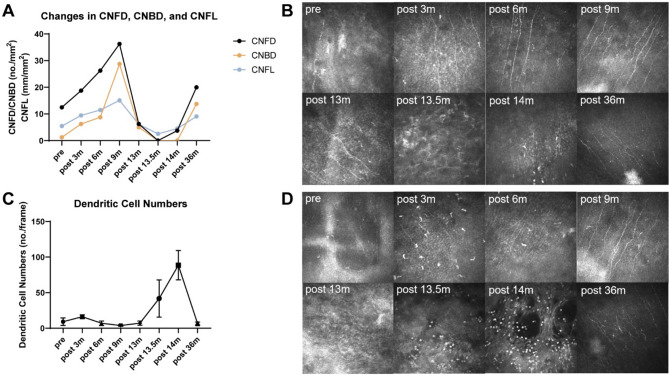
Results: A 59-year-old female presented to ophthalmology department of our hospital with facial paralysis induced by neurosurgeries. After detailed ophthalmological examination, she was diagnosed with Mackie stage III neurotrophic keratopathy (NK) in the right eye and subsequently underwent MICN and amniotic membrane transplantation. Postoperatively, corneal sensation and the epithelial defect showed gradual improvement, with corneal sensation recovering to 30 mm (measured by Cochet-Bonnet esthesiometer). However, thirteen months after MICN, she developed a corneal ulcer in the right eye one week after contracting SARS-CoV-2 (COVID-19). Supplementary investigations, including anterior segment photography, in vivo confocal microscopy (IVCM), and corneal scraping for pathogen detection, revealed recurrent corneal anesthesia and loss of corneal nerves, with no pathogens identified. After two weeks of empirical antiviral and antibacterial therapy yielded no significant improvement, a diagnosis of COVID-19-induced neurotrophic keratitis (Stage III Mackie) was established. Management consisted of prolonged medical therapy (including antiviral agents, antibiotics, nutritional supplementation, corticosteroids, and artificial tears), two amniotic membrane transplants, and one temporary tarsorrhaphy. Following two years of treatment and follow-up, the corneal lesion achieved complete healing with corneal nerve regeneration and restoration of corneal sensation.
Conclusion: This study presents the first documented case of COVID-19-related NK following MICN established as a diagnosis of exclusion. This case underscores the critical need for comprehensive differential diagnosis to rule out infectious etiologies in post-MICN keratitis, ultimately leading to a diagnosis of exclusion for COVID-19-induced disease. The diagnostic approach outlined may offer valuable insights for similar presentations. After a protracted clinical course, the patient ultimately achieved restoration of corneal sensation and reinnervation, demonstrating the preserved regenerative potential of MICN-reconstructed neural pathways even after severe viral infection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


