{"title":"The predictive utility of the E-PASS score for postoperative complications in robot-assisted partial nephrectomy: a retrospective cohort study.","authors":"Cagatay Ozsoy, Erhan Ates, Resat Inal, Mucahit Gelmis, Sahin Kilic, Mutlu Ates","doi":"10.1186/s12894-025-01899-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Robot-assisted partial nephrectomy (RAPN) is widely used for small renal tumors and provides favorable oncological and functional outcomes. However, a significant risk of postoperative complications remains a concern. Existing nephrometry scores focus on tumor anatomy but neglect patient-specific and intraoperative factors. The Estimation of Physiologic Ability and Surgical Stress (E-PASS) score, originally developed for gastrointestinal surgery, combines physiological and surgical parameters for the prediction of postoperative risk. This study evaluates the predictive performance of the E-PASS score in RAPN.</p><p><strong>Methods: </strong>This observational study retrospectively analyzed 166 patients who underwent RAPN between March 2015 and September 2024. The preoperative risk score (PRS), surgical stress score (SSS), and comprehensive risk score (CRS) were calculated. Complications developing within 30 days were classified using the Clavien-Dindo system, with Grade 2 or higher events being considered significant. The performance of the CRS in predicting postoperative complications was evaluated via receiver operating characteristic (ROC) curve analysis, while model calibration was assessed by means of a calibration plot. Logistic regression was used to identify independent predictors of postoperative complication risk. Bootstrap resampling was used to estimate 95% confidence intervals.</p><p><strong>Results: </strong>Grade 2 or higher complications occurred in 26 patients (15.7%). CRS was significantly greater in the complication group (p < 0.001). ROC analysis demonstrated good discrimination (AUC: 0.721; 95% CI: 0.629-0.812). A CRS cut-off of 0.083 yielded 76.8% sensitivity and 59.5% specificity. The calibration plot indicated good agreement between predicted and observed probabilities. Multivariate analysis identified CRS (OR: 1.537, p = 0.044), tumor size (OR: 1.048, p = 0.020), and off-clamp surgery (OR: 4.569, p = 0.003) as independent predictors.</p><p><strong>Conclusions: </strong>E-PASS CRS reliably predicts postoperative complications in RAPN and enhances risk stratification by incorporating patient-specific surgical factors. Its integration may assist more personalized perioperative management in urological surgery.</p>","PeriodicalId":9285,"journal":{"name":"BMC Urology","volume":"25 1","pages":"197"},"PeriodicalIF":1.9000,"publicationDate":"2025-08-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12335025/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Urology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12894-025-01899-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Robot-assisted partial nephrectomy (RAPN) is widely used for small renal tumors and provides favorable oncological and functional outcomes. However, a significant risk of postoperative complications remains a concern. Existing nephrometry scores focus on tumor anatomy but neglect patient-specific and intraoperative factors. The Estimation of Physiologic Ability and Surgical Stress (E-PASS) score, originally developed for gastrointestinal surgery, combines physiological and surgical parameters for the prediction of postoperative risk. This study evaluates the predictive performance of the E-PASS score in RAPN.
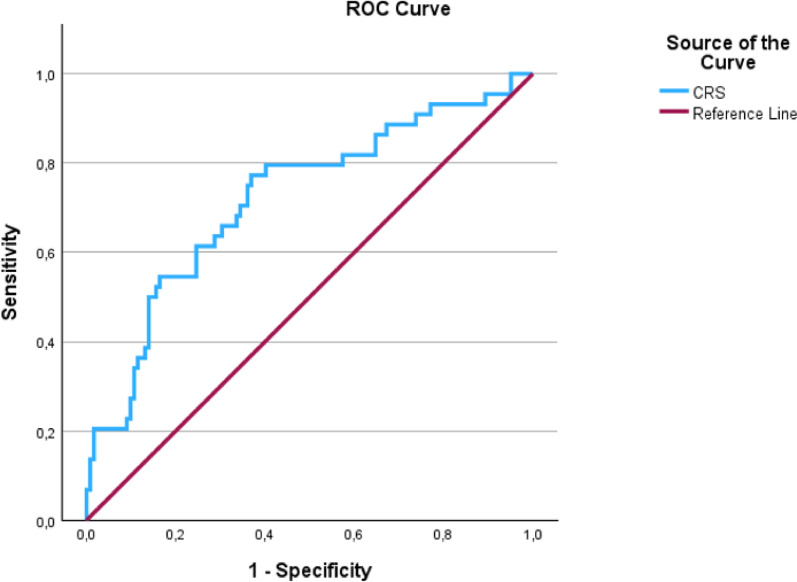
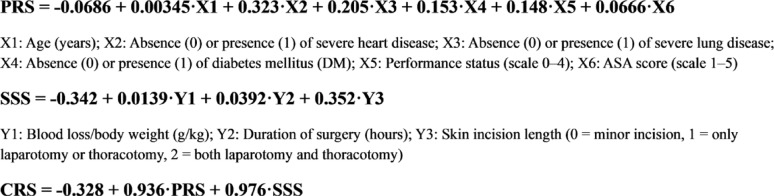
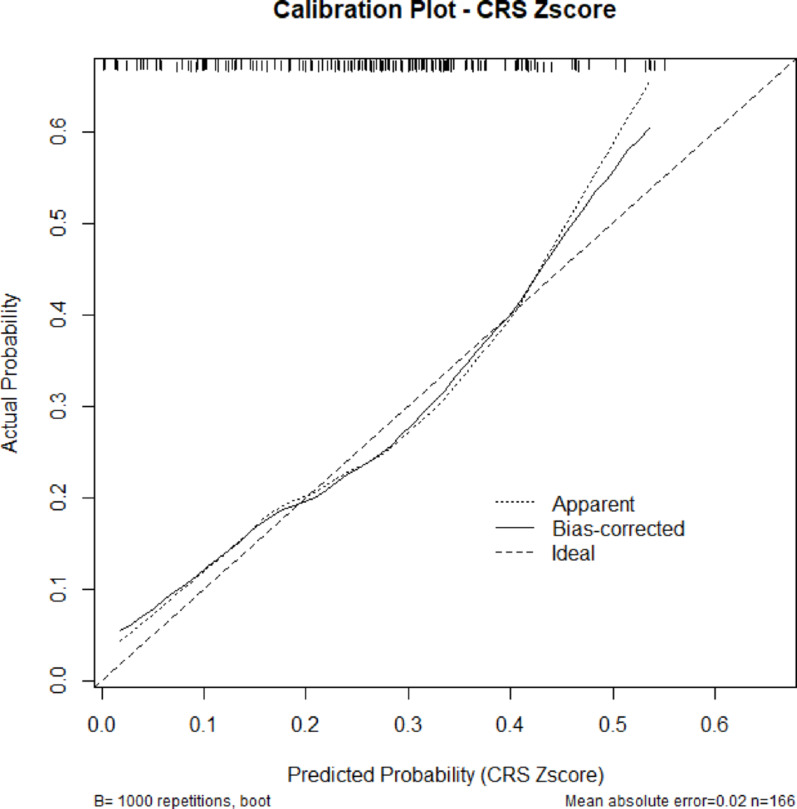
Methods: This observational study retrospectively analyzed 166 patients who underwent RAPN between March 2015 and September 2024. The preoperative risk score (PRS), surgical stress score (SSS), and comprehensive risk score (CRS) were calculated. Complications developing within 30 days were classified using the Clavien-Dindo system, with Grade 2 or higher events being considered significant. The performance of the CRS in predicting postoperative complications was evaluated via receiver operating characteristic (ROC) curve analysis, while model calibration was assessed by means of a calibration plot. Logistic regression was used to identify independent predictors of postoperative complication risk. Bootstrap resampling was used to estimate 95% confidence intervals.
Results: Grade 2 or higher complications occurred in 26 patients (15.7%). CRS was significantly greater in the complication group (p < 0.001). ROC analysis demonstrated good discrimination (AUC: 0.721; 95% CI: 0.629-0.812). A CRS cut-off of 0.083 yielded 76.8% sensitivity and 59.5% specificity. The calibration plot indicated good agreement between predicted and observed probabilities. Multivariate analysis identified CRS (OR: 1.537, p = 0.044), tumor size (OR: 1.048, p = 0.020), and off-clamp surgery (OR: 4.569, p = 0.003) as independent predictors.
Conclusions: E-PASS CRS reliably predicts postoperative complications in RAPN and enhances risk stratification by incorporating patient-specific surgical factors. Its integration may assist more personalized perioperative management in urological surgery.
期刊介绍:
BMC Urology is an open access journal publishing original peer-reviewed research articles in all aspects of the prevention, diagnosis and management of urological disorders, as well as related molecular genetics, pathophysiology, and epidemiology.
The journal considers manuscripts in the following broad subject-specific sections of urology:
Endourology and technology
Epidemiology and health outcomes
Pediatric urology
Pre-clinical and basic research
Reconstructive urology
Sexual function and fertility
Urological imaging
Urological oncology
Voiding dysfunction
Case reports.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


