{"title":"Amebic liver abscess rupture into inferior vena cava with pulmonary thrombo embolism: a case report.","authors":"Sripooja Makthala, Lovenish Bains, Pawan Lal, Kranthi Naik Bhukya","doi":"10.1186/s13256-025-05479-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Vascular complications such as hepatic vein and inferior vena cava thrombus, phlebitis, and extrahepatic biliary obstruction are rare in amebic liver abscesses. Many pathophysiological mechanisms are proposed, but the exact pathogenesis is still not known. These complications are believed to be multifactorial, with local and systemic factors acting synergistically. Here, we present a case of amebic abscess rupture into the inferior vena cava, with a thrombus extending up to the right atrium and pulmonary thromboembolism treated successfully.</p><p><strong>Case presentation: </strong>A 45-year-old Indian male presented with multiple episodes of fever with chills, palpitations, dyspnea, right upper abdominal pain, bilateral lower limb edema, and petechia for 20 days. On examination, tachycardia, tender hepatomegaly, and reduced air entry in the right lower lobe of the lung were observed. Ultrasound revealed an abscess in the left lobe of the liver about 150 cc in volume, abutting the inferior vena cava with rupture into it. Contrast-enhanced computed tomography imaging showed 5.7 × 6.2 × 5.4 cm segment IV A liver abscess with capsule breach into the intrahepatic vena cava and thrombus extending up to the right atrium was observed. Computed tomography-pulmonary angiography revealed a right atrium thrombus with bilateral pulmonary artery thrombus and parenchymal infarcts. Raised D-dimer, protein C and S deficiency was observed. The patient was managed by needle aspiration of abscess, anticoagulation, and antibiotics.</p><p><strong>Conclusion: </strong>Vascular complications need a high index of suspicion, good clinical knowledge, timely workup, and intervention. Direct rupture of an amebic liver abscess into the inferior vena cava, leading to pulmonary thromboembolism, is exceedingly rare and is not well-documented in the literature. Thorough investigation and timely intervention can successfully treat the patient.</p>","PeriodicalId":16236,"journal":{"name":"Journal of Medical Case Reports","volume":"19 1","pages":"397"},"PeriodicalIF":0.8000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12333142/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13256-025-05479-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Vascular complications such as hepatic vein and inferior vena cava thrombus, phlebitis, and extrahepatic biliary obstruction are rare in amebic liver abscesses. Many pathophysiological mechanisms are proposed, but the exact pathogenesis is still not known. These complications are believed to be multifactorial, with local and systemic factors acting synergistically. Here, we present a case of amebic abscess rupture into the inferior vena cava, with a thrombus extending up to the right atrium and pulmonary thromboembolism treated successfully.
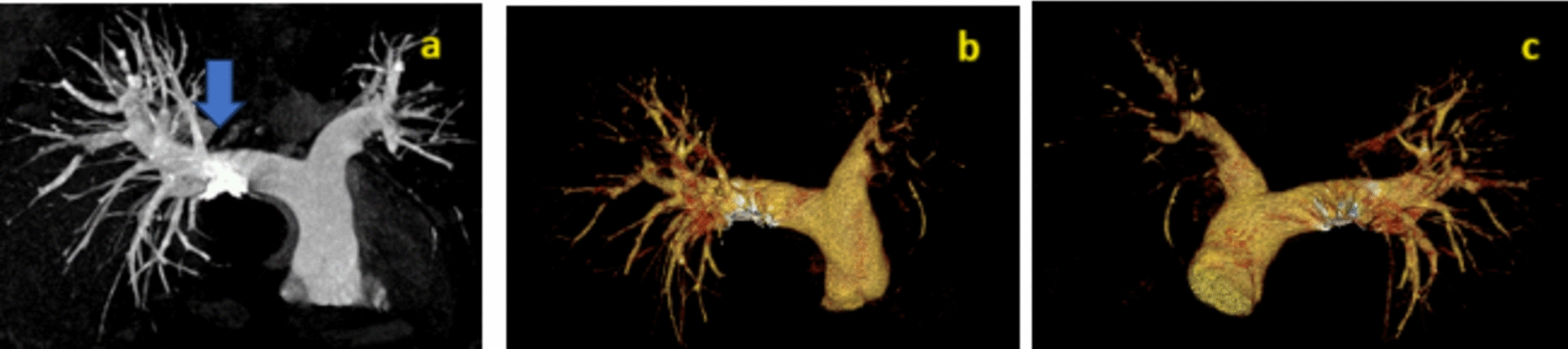
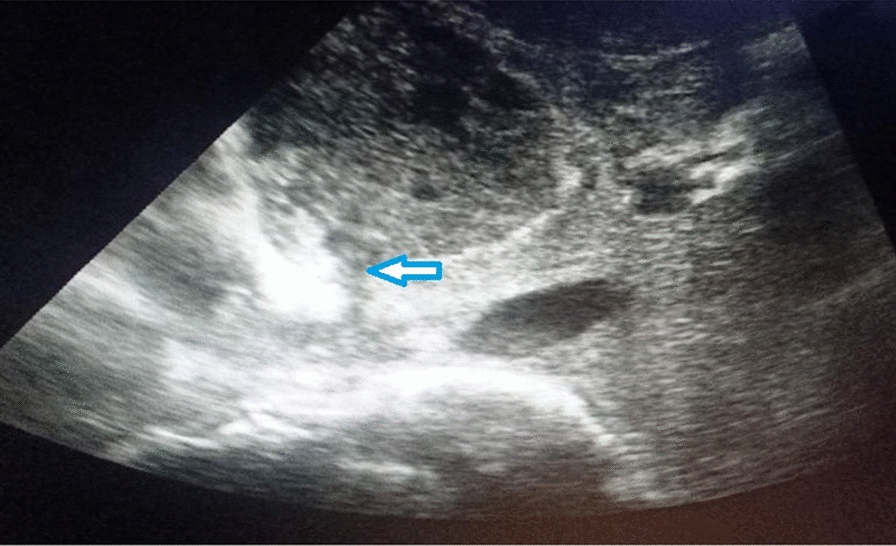
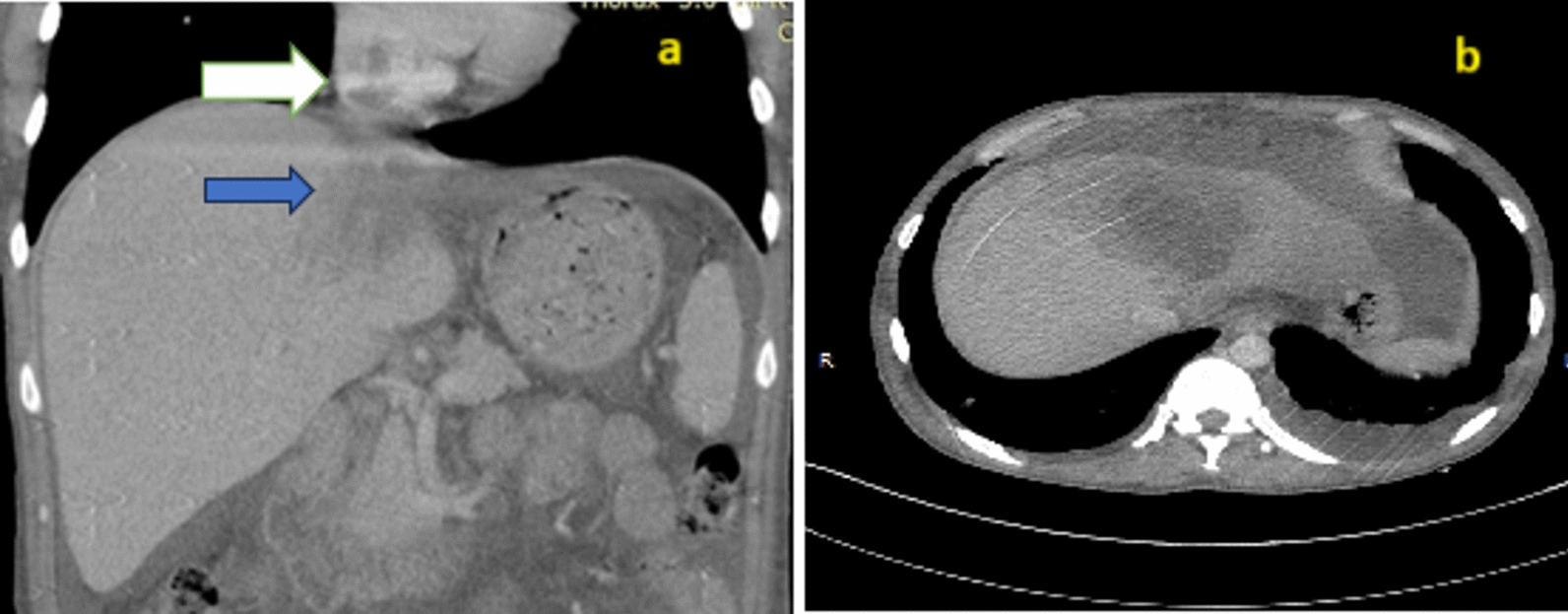
Case presentation: A 45-year-old Indian male presented with multiple episodes of fever with chills, palpitations, dyspnea, right upper abdominal pain, bilateral lower limb edema, and petechia for 20 days. On examination, tachycardia, tender hepatomegaly, and reduced air entry in the right lower lobe of the lung were observed. Ultrasound revealed an abscess in the left lobe of the liver about 150 cc in volume, abutting the inferior vena cava with rupture into it. Contrast-enhanced computed tomography imaging showed 5.7 × 6.2 × 5.4 cm segment IV A liver abscess with capsule breach into the intrahepatic vena cava and thrombus extending up to the right atrium was observed. Computed tomography-pulmonary angiography revealed a right atrium thrombus with bilateral pulmonary artery thrombus and parenchymal infarcts. Raised D-dimer, protein C and S deficiency was observed. The patient was managed by needle aspiration of abscess, anticoagulation, and antibiotics.
Conclusion: Vascular complications need a high index of suspicion, good clinical knowledge, timely workup, and intervention. Direct rupture of an amebic liver abscess into the inferior vena cava, leading to pulmonary thromboembolism, is exceedingly rare and is not well-documented in the literature. Thorough investigation and timely intervention can successfully treat the patient.
期刊介绍:
JMCR is an open access, peer-reviewed online journal that will consider any original case report that expands the field of general medical knowledge. Reports should show one of the following: 1. Unreported or unusual side effects or adverse interactions involving medications 2. Unexpected or unusual presentations of a disease 3. New associations or variations in disease processes 4. Presentations, diagnoses and/or management of new and emerging diseases 5. An unexpected association between diseases or symptoms 6. An unexpected event in the course of observing or treating a patient 7. Findings that shed new light on the possible pathogenesis of a disease or an adverse effect

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


