Amany F Elbehairy, Josephine H Naish, Hossein Baghertash, Geoff J M Parker, Christopher A Miller, Jørgen Vestbo, Alex R Horsley
{"title":"T<sub>2</sub>*-weighted oxygen-enhanced pulmonary MRI in COPD is linked to resting and exertional functional measurements.","authors":"Amany F Elbehairy, Josephine H Naish, Hossein Baghertash, Geoff J M Parker, Christopher A Miller, Jørgen Vestbo, Alex R Horsley","doi":"10.1136/bmjresp-2024-002784","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>T<sub>2</sub>*-weighted oxygen-enhanced MRI (T<sub>2</sub>*-OE-MRI) may directly assess pulmonary ventilation using oxygen as an inhaled tracer gas. It has shown promise in healthy volunteers (HVs) and cystic fibrosis but has yet to be demonstrated in patients with chronic obstructive pulmonary disease (COPD).</p><p><strong>Research question: </strong>To determine the feasibility and repeatability of T<sub>2</sub>*-OE-MRI in patients with COPD. To assess correlations between T<sub>2</sub>*-OE-MRI measurements of pulmonary ventilation, pulmonary function tests (PFTs) and measures of functional limitation.</p><p><strong>Study design and methods: </strong>13 patients with mild-to-severe COPD and 13 HVs underwent PFTs, lung clearance index (LCI) measurement, incremental exercise test (patients only) and two lung MRI scans at 3 T. For T<sub>2</sub>*-OE-MRI, participants were fitted with a non-rebreathing face mask and given 100% oxygen during image acquisition.</p><p><strong>Results: </strong>Patients (age: 63 (55-72) years, forced expiratory volume in 1 s (FEV<sub>1</sub>): 63 (36-79) %predicted, median (IQR)) had evidence of pulmonary gas trapping, small airway disease (SAD) and ventilation heterogeneity. During T<sub>2</sub>*-OE-MRI, the magnitude of the percentage difference between mean signal intensity at normoxia and hyperoxia (percent signal enhancement (PSE)) and the enhancing fraction (EF) were lower in patients versus HVs (2.77 (2.19-4.19) vs 5.34 (4.33-5.61) % and 0.74 (0.66-0.77) vs 0.89 (0.82-0.94), respectively, both p<0.001). Intraclass correlation coefficient values indicated moderate (0.74) and good (0.80) repeatability for PSE and EF, respectively. PSE and EF significantly correlated with FEV<sub>1</sub>, LCI and SAD indices, and in COPD, they correlated with measures of exercise capacity, dynamic hyperinflation and dyspnoea intensity during exercise.</p><p><strong>Interpretation: </strong>In patients with COPD, T<sub>2</sub>*-OE-MRI is feasible and repeatable and provides regional information on pulmonary ventilation that is linked with physiological measures of disease severity, functional limitation and exertional dyspnoea.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"12 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12336524/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2024-002784","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
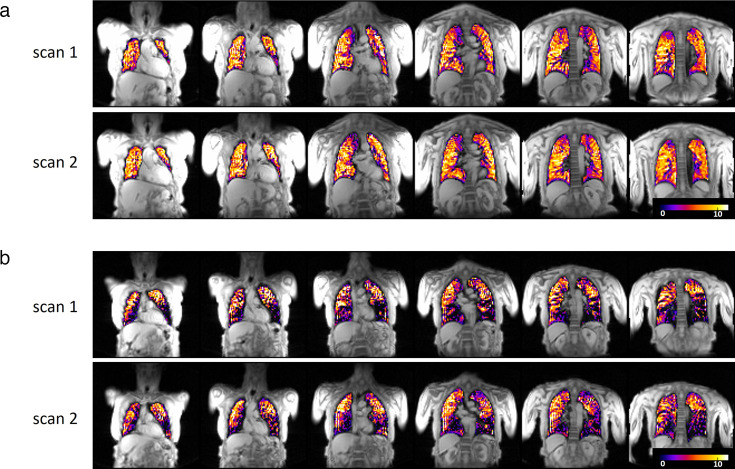
Background: T2*-weighted oxygen-enhanced MRI (T2*-OE-MRI) may directly assess pulmonary ventilation using oxygen as an inhaled tracer gas. It has shown promise in healthy volunteers (HVs) and cystic fibrosis but has yet to be demonstrated in patients with chronic obstructive pulmonary disease (COPD).
Research question: To determine the feasibility and repeatability of T2*-OE-MRI in patients with COPD. To assess correlations between T2*-OE-MRI measurements of pulmonary ventilation, pulmonary function tests (PFTs) and measures of functional limitation.
Study design and methods: 13 patients with mild-to-severe COPD and 13 HVs underwent PFTs, lung clearance index (LCI) measurement, incremental exercise test (patients only) and two lung MRI scans at 3 T. For T2*-OE-MRI, participants were fitted with a non-rebreathing face mask and given 100% oxygen during image acquisition.
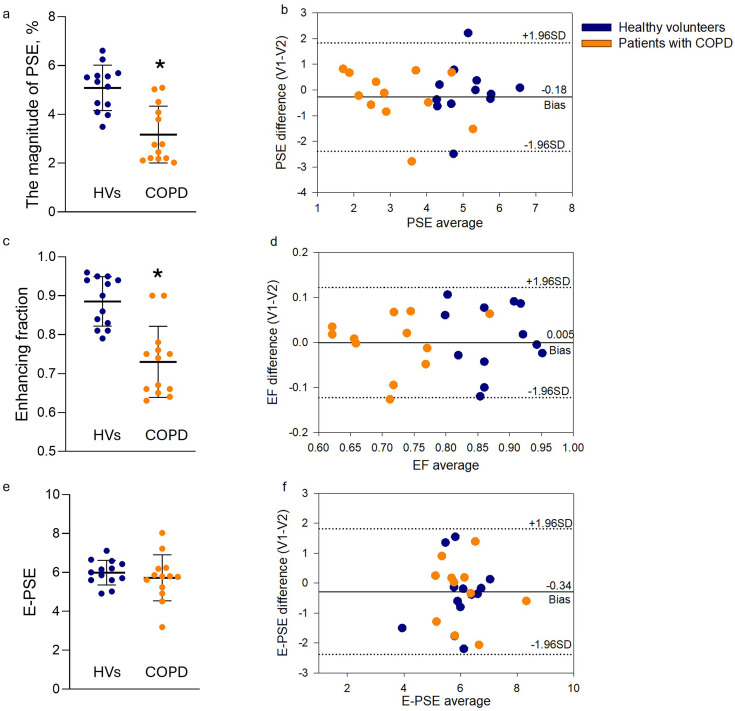
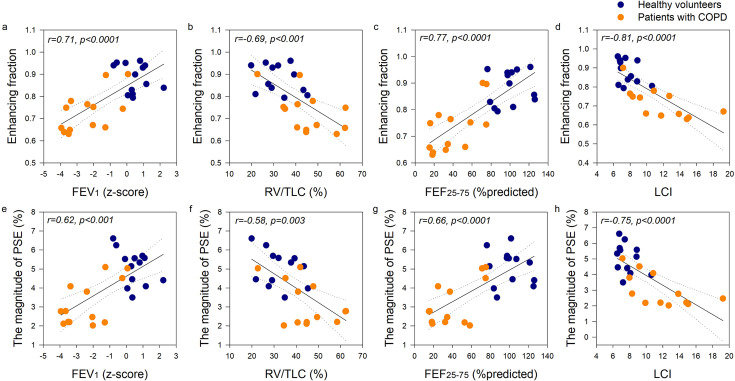
Results: Patients (age: 63 (55-72) years, forced expiratory volume in 1 s (FEV1): 63 (36-79) %predicted, median (IQR)) had evidence of pulmonary gas trapping, small airway disease (SAD) and ventilation heterogeneity. During T2*-OE-MRI, the magnitude of the percentage difference between mean signal intensity at normoxia and hyperoxia (percent signal enhancement (PSE)) and the enhancing fraction (EF) were lower in patients versus HVs (2.77 (2.19-4.19) vs 5.34 (4.33-5.61) % and 0.74 (0.66-0.77) vs 0.89 (0.82-0.94), respectively, both p<0.001). Intraclass correlation coefficient values indicated moderate (0.74) and good (0.80) repeatability for PSE and EF, respectively. PSE and EF significantly correlated with FEV1, LCI and SAD indices, and in COPD, they correlated with measures of exercise capacity, dynamic hyperinflation and dyspnoea intensity during exercise.
Interpretation: In patients with COPD, T2*-OE-MRI is feasible and repeatable and provides regional information on pulmonary ventilation that is linked with physiological measures of disease severity, functional limitation and exertional dyspnoea.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


