CT-based radiomics model for noninvasive prediction of progression-free survival in high-grade serous ovarian carcinoma: a multicenter study incorporating preoperative and postoperative clinical factors.
IF 3.2 3区 医学Q2 RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
{"title":"CT-based radiomics model for noninvasive prediction of progression-free survival in high-grade serous ovarian carcinoma: a multicenter study incorporating preoperative and postoperative clinical factors.","authors":"Xinping Yu, Zidong Zhang, Yuwei Zou, Chang Wang, Jinwen Jiao, Chengjian Wang, Haiyang Yu, Shuai Zhang","doi":"10.1186/s12880-025-01865-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To investigate the potential of combining radiomics with clinicoradiological features in predicting progression-free survival (PFS) after the surgery of high-grade serous ovarian carcinoma (HGSOC).</p><p><strong>Methods: </strong>In this retrospective multicenter study, a total of 195 patients with pathologically confirmed HGSOC who underwent cytoreductive surgery followed by platinum-based chemotherapy were included from two institutions (train cohort, n = 134; test cohort, n = 61). From the train cohort, univariate and multivariate Cox proportional hazards regression analyses systematically evaluated associations between clinicoradiological features and PFS, culminating in a clinical prediction model for stratifying progression risk. Radiomics features were extracted and utilized to build the radiomics model through univariate Cox regression and least absolute shrinkage and selection operator Cox regression. A combined model integrating both clinicoradiological and radiomics features was subsequently developed. The concordance index (C-index) was used to assess the predictive performance of different models in 1-, 3-, and 5-year PFS evens among HGSOC patients. Model performance was assessed using time-dependent receiver operating characteristic curves, with area under the curve (AUC) values calculated at various time points. as well as calibration curves and Brier scores to evaluate prediction accuracy and model reliability. Kaplan-Meier analysis was employed to evaluate the clinical utility of each model in predicting PFS.</p><p><strong>Results: </strong>Five clinicoradiologicall features, including supradiaphragmatic lymphadenopathy, CA125 level, HE4 level, residual tumor status, and FIGO stage, were included in the clinical model.The combined model achieved strong predictive performance with a C-index of 0.758 (95% CI: 0.685-0.830) in the train cohort and 0.707 (95% CI: 0.593-0.821) in the test cohort, outperforming both the clinical and radiomics models independently. The combined model demonstrated superior performance for 1-year prediction, with the highest accuracy (0.822), AUC (0.864), and lowest Brier score (0.132) in the train cohort, and the highest balanced accuracy (0.806), AUC (0.787), and lowest Brier score (0.159) in the test cohort. For 3-year survival, the radiomics model showed the best performance, with a balanced accuracy of 0.760, AUC of 0.838, and Brier score of 0.168 in train cohort, and a balanced accuracy of 0.813, AUC of 0.785, and Brier score of 0.198 in test cohort. Similarly, the radiomics model overall outperformed the other models for 5-year survival, with a balanced accuracy of 0.813, AUC of 0.887, and Brier score of 0.164 in train cohort, and a balanced accuracy of 0.813, AUC of 0.767, and Brier score of 0.207 in test cohort.</p><p><strong>Conclusion: </strong>The combined model excels in 1-year PFS prediction and overall risk stratification, while the radiomics model performs better for 3- and 5-year fixed-time PFS predictions.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>","PeriodicalId":9020,"journal":{"name":"BMC Medical Imaging","volume":"25 1","pages":"320"},"PeriodicalIF":3.2000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12335143/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Medical Imaging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12880-025-01865-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To investigate the potential of combining radiomics with clinicoradiological features in predicting progression-free survival (PFS) after the surgery of high-grade serous ovarian carcinoma (HGSOC).
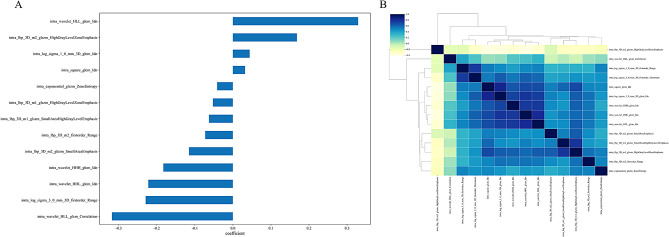
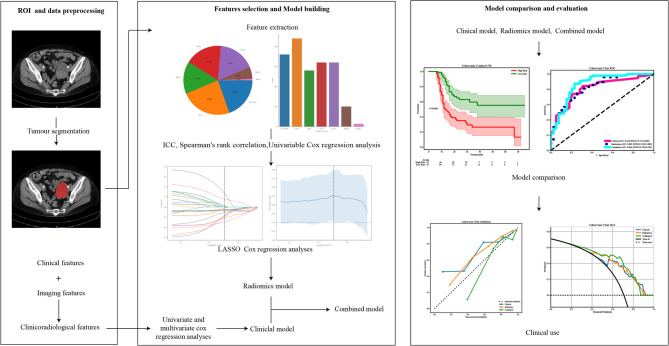
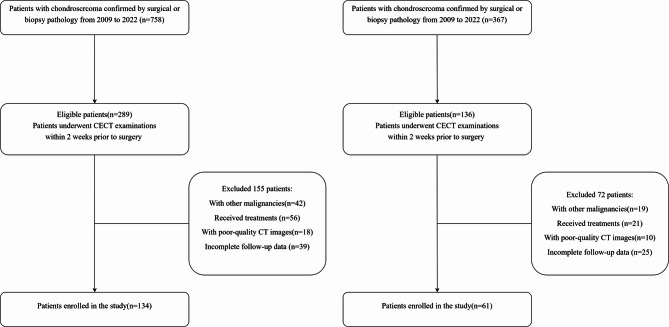
Methods: In this retrospective multicenter study, a total of 195 patients with pathologically confirmed HGSOC who underwent cytoreductive surgery followed by platinum-based chemotherapy were included from two institutions (train cohort, n = 134; test cohort, n = 61). From the train cohort, univariate and multivariate Cox proportional hazards regression analyses systematically evaluated associations between clinicoradiological features and PFS, culminating in a clinical prediction model for stratifying progression risk. Radiomics features were extracted and utilized to build the radiomics model through univariate Cox regression and least absolute shrinkage and selection operator Cox regression. A combined model integrating both clinicoradiological and radiomics features was subsequently developed. The concordance index (C-index) was used to assess the predictive performance of different models in 1-, 3-, and 5-year PFS evens among HGSOC patients. Model performance was assessed using time-dependent receiver operating characteristic curves, with area under the curve (AUC) values calculated at various time points. as well as calibration curves and Brier scores to evaluate prediction accuracy and model reliability. Kaplan-Meier analysis was employed to evaluate the clinical utility of each model in predicting PFS.
Results: Five clinicoradiologicall features, including supradiaphragmatic lymphadenopathy, CA125 level, HE4 level, residual tumor status, and FIGO stage, were included in the clinical model.The combined model achieved strong predictive performance with a C-index of 0.758 (95% CI: 0.685-0.830) in the train cohort and 0.707 (95% CI: 0.593-0.821) in the test cohort, outperforming both the clinical and radiomics models independently. The combined model demonstrated superior performance for 1-year prediction, with the highest accuracy (0.822), AUC (0.864), and lowest Brier score (0.132) in the train cohort, and the highest balanced accuracy (0.806), AUC (0.787), and lowest Brier score (0.159) in the test cohort. For 3-year survival, the radiomics model showed the best performance, with a balanced accuracy of 0.760, AUC of 0.838, and Brier score of 0.168 in train cohort, and a balanced accuracy of 0.813, AUC of 0.785, and Brier score of 0.198 in test cohort. Similarly, the radiomics model overall outperformed the other models for 5-year survival, with a balanced accuracy of 0.813, AUC of 0.887, and Brier score of 0.164 in train cohort, and a balanced accuracy of 0.813, AUC of 0.767, and Brier score of 0.207 in test cohort.
Conclusion: The combined model excels in 1-year PFS prediction and overall risk stratification, while the radiomics model performs better for 3- and 5-year fixed-time PFS predictions.
期刊介绍:
BMC Medical Imaging is an open access journal publishing original peer-reviewed research articles in the development, evaluation, and use of imaging techniques and image processing tools to diagnose and manage disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


