Predictive value of left ventricular myocardial constructive work in patients with heart failure with preserved ejection fraction and preclinical diastolic dysfunction.
{"title":"Predictive value of left ventricular myocardial constructive work in patients with heart failure with preserved ejection fraction and preclinical diastolic dysfunction.","authors":"Aram Chilingaryan, Lusine Tunyan, Milena Arzumanyan, Hovik Balyan","doi":"10.1186/s44348-025-00053-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We aimed to find predictors of ejection fraction (EF) deterioration in heart failure with preserved EF (HFpEF) patients to prevent their further deterioration.</p><p><strong>Methods: </strong>We studied 215 patients (mean age, 73 ± 8 years; 63% women) with HFpEF and with records of Charlson Comorbidity Index, glomerular filtration rate. Myocardial work, global longitudinal, radial, circumferential, and area strain. The global work index, global constructive work (GCW), wasted work, global work efficiency was obtained by echocardiography. Patients were followed up for 3 years.</p><p><strong>Results: </strong>Five patients developed myocardial infarction and were excluded from the study. Baseline EF was higher in female patients (61.2% ± 3.1% vs. 56.4% ± 2.7%, P < 0.002), in patients aged > 70 years (62.4% ± 2.1% vs. 57.1% ± 2.3%, P < 0.005), and in patients with end-diastolic volume index < 60 mL/m<sup>2</sup> (56.1% ± 3.2% vs. 63.4% ± 2.3%, P < 0.001). EF decline compared to baseline was -7.3% ± 1.6% (P < 0.01). EF decline was significantly more in patients aged > 70 years, in patients with coronary artery disease and did not relate to sex, left ventricle size, cardiac index, and glomerular filtration rate. During follow-up 58 patients (27%) had EF < 50%, worsening in area strain (-27.9% ± 8.5% vs. -24.7% ± 5.3%, P < 0.003), global longitudinal strain (-19.7% ± 2.4% vs. -17.1% ± 1.6%, P < 0.005), and GCW (2,378% ± 117% vs. 2,102% ± 10%, P < 0.002). Patients with EF < 50% at the end of the study had less area strain and GCW baseline values compared with patients with EF > 50% (22.4% ± 7.2% vs. -27.6% ± 8.1%, P < 0.002; 2,081 ± 92 vs. 2,489 ± 127, P < 0.001). GCW was the predictor of EF deterioration (area under curve, 0.8853).</p><p><strong>Conclusions: </strong>GCW predicts EF decline in HFpEF patients which may help identify this subset of patients and prevent their further deterioration earlier.</p>","PeriodicalId":15229,"journal":{"name":"Journal of Cardiovascular Imaging","volume":"33 1","pages":"11"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12333278/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Imaging","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44348-025-00053-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: We aimed to find predictors of ejection fraction (EF) deterioration in heart failure with preserved EF (HFpEF) patients to prevent their further deterioration.
Methods: We studied 215 patients (mean age, 73 ± 8 years; 63% women) with HFpEF and with records of Charlson Comorbidity Index, glomerular filtration rate. Myocardial work, global longitudinal, radial, circumferential, and area strain. The global work index, global constructive work (GCW), wasted work, global work efficiency was obtained by echocardiography. Patients were followed up for 3 years.
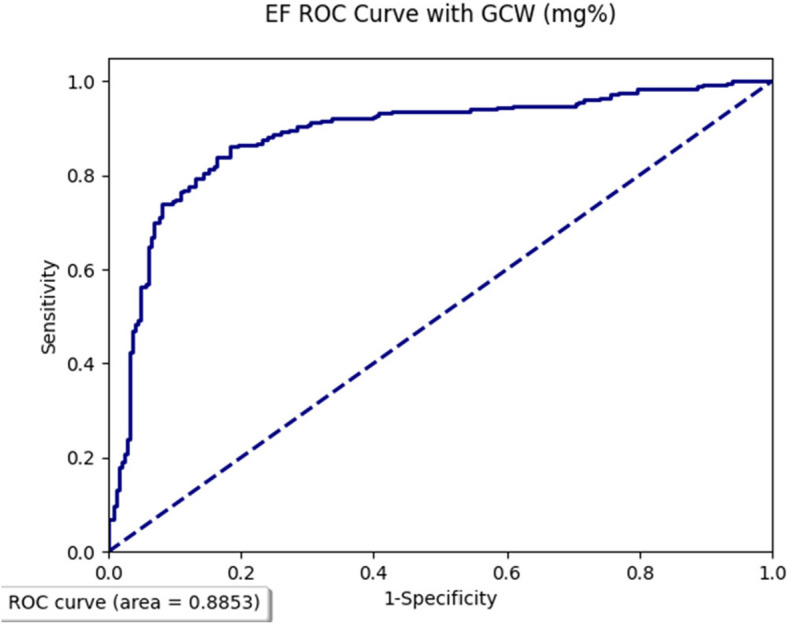
Results: Five patients developed myocardial infarction and were excluded from the study. Baseline EF was higher in female patients (61.2% ± 3.1% vs. 56.4% ± 2.7%, P < 0.002), in patients aged > 70 years (62.4% ± 2.1% vs. 57.1% ± 2.3%, P < 0.005), and in patients with end-diastolic volume index < 60 mL/m2 (56.1% ± 3.2% vs. 63.4% ± 2.3%, P < 0.001). EF decline compared to baseline was -7.3% ± 1.6% (P < 0.01). EF decline was significantly more in patients aged > 70 years, in patients with coronary artery disease and did not relate to sex, left ventricle size, cardiac index, and glomerular filtration rate. During follow-up 58 patients (27%) had EF < 50%, worsening in area strain (-27.9% ± 8.5% vs. -24.7% ± 5.3%, P < 0.003), global longitudinal strain (-19.7% ± 2.4% vs. -17.1% ± 1.6%, P < 0.005), and GCW (2,378% ± 117% vs. 2,102% ± 10%, P < 0.002). Patients with EF < 50% at the end of the study had less area strain and GCW baseline values compared with patients with EF > 50% (22.4% ± 7.2% vs. -27.6% ± 8.1%, P < 0.002; 2,081 ± 92 vs. 2,489 ± 127, P < 0.001). GCW was the predictor of EF deterioration (area under curve, 0.8853).
Conclusions: GCW predicts EF decline in HFpEF patients which may help identify this subset of patients and prevent their further deterioration earlier.
背景:我们的目的是寻找心力衰竭保留EF (HFpEF)患者射血分数恶化的预测因素,以防止其进一步恶化。方法:研究215例患者(平均年龄73±8岁;(63%女性)HFpEF,并有Charlson合并症指数、肾小球滤过率记录。心肌功,整体纵向,径向,周向和区域应变。通过超声心动图获得总工作指数、总建设性工作、浪费工作、总工作效率。患者随访3年。结果:5例患者发生心肌梗死,被排除在研究之外。基线EF在女性患者中(61.2%±3.1% vs. 56.4%±2.7%,p70年)高于冠心病患者(62.4%±2.1% vs. 57.1%±2.3%,p2(56.1%±3.2% vs. 63.4%±2.3%,p70年),且与性别、左心室大小、心脏指数和肾小球滤过率无关。在随访期间,58例(27%)患者EF为50%(22.4%±7.2% vs -27.6%±8.1%)。结论:GCW预测HFpEF患者EF下降,可能有助于识别这类患者并早期预防其进一步恶化。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


