Can preoperative CT angiography and three-dimensional reconstruction of the mesenteric artery of the colon improve laparoscopic colectomy and postoperative rehabilitation in patients with colon cancer? A pilot randomized control study.
Peng Zhang, Jun Luo, Jiehui Huang, Jingjing Sun, Haiyang Feng, Yuping Zhu, Yong Liu
{"title":"Can preoperative CT angiography and three-dimensional reconstruction of the mesenteric artery of the colon improve laparoscopic colectomy and postoperative rehabilitation in patients with colon cancer? A pilot randomized control study.","authors":"Peng Zhang, Jun Luo, Jiehui Huang, Jingjing Sun, Haiyang Feng, Yuping Zhu, Yong Liu","doi":"10.1007/s00384-025-04975-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To assess the effect of computed tomography angiography (CTA) and three-dimensional (3D) reconstruction on laparoscopic colectomy in patients with colon cancer.</p><p><strong>Methods: </strong>Patients with colon cancer who were treated at Zhejiang Cancer Hospital between August 2020 and December 2022 were included in this pilot, randomized controlled trial. The participants were randomly assigned to either the CTA group, in which patients underwent preoperative CTA and 3D reconstruction, or the control group, in which patients underwent preoperative enhanced abdominal and pelvic CT examinations. The primary outcome was the duration of the operation. The secondary outcomes included intraoperative blood loss, length of hospital stay, number of lymph node dissections, fasting duration, duration of tube drainage, overall survival (OS), and progression-free survival (PFS). To minimize statistical bias, patients were stratified into subgroups on the basis of tumor location (left colon or right colon). Additionally, variations in the middle colonic artery (MCA), inferior mesenteric artery (IMA), and colonic branches of superior mesenteric artery (cbSMA) classifications were documented.</p><p><strong>Results: </strong>A total of 82 patients (41 in each group) were included in the analysis. The CTA group had significantly shorter operation durations (123.68 ± 26.09 vs. 154.12 ± 33.15 min, P < 0.001) and fasting durations (median 4.00 vs. 5.00 days, P < 0.001) as well as reduced intraoperative blood loss (median 50.00 vs. 100.00 mL, P = 0.001) compared to the control group; these differences were observed in the overall colon cancer cohort and in the left and right colon subgroups. However, no significant differences were observed between the two groups in terms of lymph node dissection, tube drainage duration, hospitalization duration, OS or PFS. In the CTA group, the proportions of patients with different IMA types were as follows: Type A (60.97%), Type B (9.76%), Type C (17.07%), and Type D (12.20%); the proportions of patients with different MCA types were as follows: Type A (78.05%), Type B (12.20%), Type C (7.31%), and Type D (2.44%); and the proportions of patients with different cbSMA types were as follows: Type A (65.85%), Type B (7.32%), Type C (17.07%), and Type D (9.76%). Patients with a tumor size ≥ 5 cm, preoperative intestinal obstruction, postoperative pathological serosal invasion, lymph node metastasis, and stage III disease had significantly worse OS and PFS than those with a tumor size < 5 cm (P = 0.007, P = 0.026), no preoperative intestinal obstruction (P = 0.015, P = 0.019), no serosal invasion (P = 0.001, P = 0.001), no lymph node metastasis (P = 0.016, P = 0.001), and stage I-II disease (P = 0.013, P = 0.001). However, no significant differences in OS or PFS were observed between patients who underwent preoperative CTA examination and the control group (P = 0.551, P = 0.591), between male and female patients (P = 0.402, P = 0.361), or between patients with and without postoperative complications (P = 0.561, P = 0.520). Finally, multivariate Cox proportional hazards regression analysis revealed that serosal invasion (P = 0.013; P = 0.009), lymph node metastasis (P = 0.029; P = 0.043), and tumor stage (P = 0.002; P = 0.001) were independent prognostic factors that affected the OS and PFS of patients with colon cancer.</p><p><strong>Conclusion: </strong>Preoperative CTA and 3D reconstruction provide essential information for laparoscopic surgery, facilitate the optimization of surgical procedures, and support improved postoperative recovery for patients with colon cancer, suggesting promising clinical applications.</p>","PeriodicalId":13789,"journal":{"name":"International Journal of Colorectal Disease","volume":"40 1","pages":"173"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12334536/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Colorectal Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00384-025-04975-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To assess the effect of computed tomography angiography (CTA) and three-dimensional (3D) reconstruction on laparoscopic colectomy in patients with colon cancer.
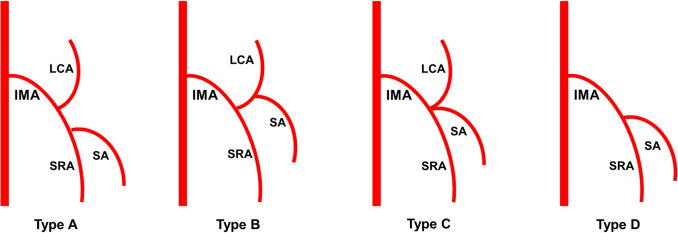
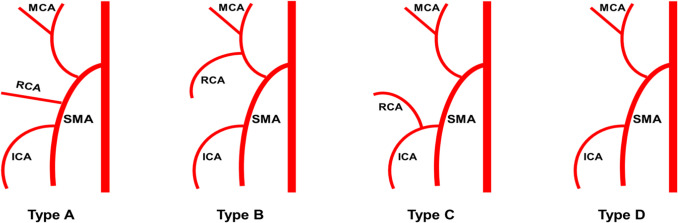
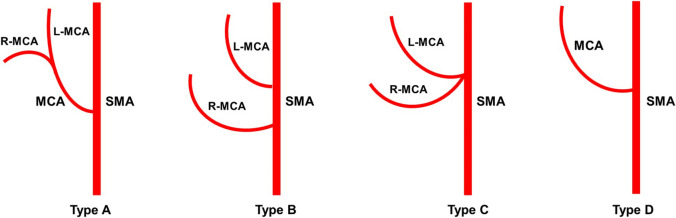
Methods: Patients with colon cancer who were treated at Zhejiang Cancer Hospital between August 2020 and December 2022 were included in this pilot, randomized controlled trial. The participants were randomly assigned to either the CTA group, in which patients underwent preoperative CTA and 3D reconstruction, or the control group, in which patients underwent preoperative enhanced abdominal and pelvic CT examinations. The primary outcome was the duration of the operation. The secondary outcomes included intraoperative blood loss, length of hospital stay, number of lymph node dissections, fasting duration, duration of tube drainage, overall survival (OS), and progression-free survival (PFS). To minimize statistical bias, patients were stratified into subgroups on the basis of tumor location (left colon or right colon). Additionally, variations in the middle colonic artery (MCA), inferior mesenteric artery (IMA), and colonic branches of superior mesenteric artery (cbSMA) classifications were documented.
Results: A total of 82 patients (41 in each group) were included in the analysis. The CTA group had significantly shorter operation durations (123.68 ± 26.09 vs. 154.12 ± 33.15 min, P < 0.001) and fasting durations (median 4.00 vs. 5.00 days, P < 0.001) as well as reduced intraoperative blood loss (median 50.00 vs. 100.00 mL, P = 0.001) compared to the control group; these differences were observed in the overall colon cancer cohort and in the left and right colon subgroups. However, no significant differences were observed between the two groups in terms of lymph node dissection, tube drainage duration, hospitalization duration, OS or PFS. In the CTA group, the proportions of patients with different IMA types were as follows: Type A (60.97%), Type B (9.76%), Type C (17.07%), and Type D (12.20%); the proportions of patients with different MCA types were as follows: Type A (78.05%), Type B (12.20%), Type C (7.31%), and Type D (2.44%); and the proportions of patients with different cbSMA types were as follows: Type A (65.85%), Type B (7.32%), Type C (17.07%), and Type D (9.76%). Patients with a tumor size ≥ 5 cm, preoperative intestinal obstruction, postoperative pathological serosal invasion, lymph node metastasis, and stage III disease had significantly worse OS and PFS than those with a tumor size < 5 cm (P = 0.007, P = 0.026), no preoperative intestinal obstruction (P = 0.015, P = 0.019), no serosal invasion (P = 0.001, P = 0.001), no lymph node metastasis (P = 0.016, P = 0.001), and stage I-II disease (P = 0.013, P = 0.001). However, no significant differences in OS or PFS were observed between patients who underwent preoperative CTA examination and the control group (P = 0.551, P = 0.591), between male and female patients (P = 0.402, P = 0.361), or between patients with and without postoperative complications (P = 0.561, P = 0.520). Finally, multivariate Cox proportional hazards regression analysis revealed that serosal invasion (P = 0.013; P = 0.009), lymph node metastasis (P = 0.029; P = 0.043), and tumor stage (P = 0.002; P = 0.001) were independent prognostic factors that affected the OS and PFS of patients with colon cancer.
Conclusion: Preoperative CTA and 3D reconstruction provide essential information for laparoscopic surgery, facilitate the optimization of surgical procedures, and support improved postoperative recovery for patients with colon cancer, suggesting promising clinical applications.
目的:探讨ct血管造影(CTA)和三维重建技术在结肠癌腹腔镜结肠切除术中的应用价值。方法:选取2020年8月至2022年12月在浙江省肿瘤医院接受治疗的结肠癌患者,进行随机对照试验。参与者被随机分配到CTA组,患者接受术前CTA和3D重建,或对照组,患者接受术前增强腹部和盆腔CT检查。主要结果是手术的持续时间。次要结果包括术中出血量、住院时间、淋巴结清扫次数、禁食时间、管引流时间、总生存期(OS)和无进展生存期(PFS)。为了减少统计偏差,根据肿瘤位置(左结肠或右结肠)将患者分层为亚组。此外,还记录了结肠中动脉(MCA)、肠系膜下动脉(IMA)和肠系膜上动脉(cbSMA)结肠分支分类的变化。结果:共纳入82例患者,每组41例。CTA组手术时间明显缩短(123.68±26.09 min vs. 154.12±33.15 min), P结论:术前CTA和3D重建为腹腔镜手术提供了必要的信息,有助于优化手术流程,促进结肠癌患者术后恢复,具有良好的临床应用前景。
期刊介绍:
The International Journal of Colorectal Disease, Clinical and Molecular Gastroenterology and Surgery aims to publish novel and state-of-the-art papers which deal with the physiology and pathophysiology of diseases involving the entire gastrointestinal tract. In addition to original research articles, the following categories will be included: reviews (usually commissioned but may also be submitted), case reports, letters to the editor, and protocols on clinical studies.
The journal offers its readers an interdisciplinary forum for clinical science and molecular research related to gastrointestinal disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


