Randomized single-dose crossover comparative bioavailability study of two novel oral cannabidiol (CBD) formulations in healthy volunteers under fed conditions, compared to a standard CBD isolate capsule.
Mehmet Nevzat Pisak, Edibe Bereket, Aydin Erenmemisoglu
{"title":"Randomized single-dose crossover comparative bioavailability study of two novel oral cannabidiol (CBD) formulations in healthy volunteers under fed conditions, compared to a standard CBD isolate capsule.","authors":"Mehmet Nevzat Pisak, Edibe Bereket, Aydin Erenmemisoglu","doi":"10.1186/s42238-025-00312-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study aimed to compare the pharmacokinetics and relative bioavailability of two novel cannabidiol (CBD) formulations including bioavailability-enhanced capsule (CBDNEXT Supra capsule) and a bioavailability-enhanced liquid (CBDNEXT Supra liquid)- against a standard high-purity CBD isolate capsule in healthy volunteers under fed (low-fat) conditions.</p><p><strong>Methods: </strong>A single-dose, open-label, randomized, three-period, three-sequence crossover trial was conducted in 12 healthy male volunteers (18-50 years). Of the 12 enrolled subjects, 9 completed all three treatment periods per protocol. Each received 40 mg of CBD as one of three formulations: Test-1 (enhanced CBD capsule), Test-2 (enhanced CBD liquid), or Reference (unformulated CBD isolate capsule with microcrystalline cellulose only as excipient), with a washout of 14 days between treatments. All doses were administered 30 min after a standardized low-fat (~ 300-350 kcal, < 10 g fat) breakfast to minimize the impact of dietary fat on CBD absorption. Blood samples were collected up to 72 h post-dose for plasma CBD and 7-hydroxy-CBD analysis by a validated LC-MS/MS method (LLOQ 0.1 ng/mL). Pharmacokinetic (PK) parameters (C_max, tmax, AUC_0-72, and t_1/2) were determined by non-compartmental analysis. Safety was assessed by adverse events (AEs), vital signs, and laboratory tests (including liver enzymes). Plasma cortisol was measured pre-dose and at 2-, 4-, and 8-hours post-dose as an exploratory pharmacodynamic marker.</p><p><strong>Results: </strong>Nine subjects completed all treatments (three withdrew: two for positive drug screens and one for an intercurrent moderate infection). Mean plasma CBD concentration-time profiles for the three formulations demonstrated markedly different absorption kinetics. The enhanced capsule achieved the highest peak CBD concentration (C_max 14.1 ng/mL) and exposure (AUC_0-72 38.0 h·ng/mL), compared to the enhanced liquid (C_max 6.2 ng/mL, AUC_0-72 20.2 h·ng/mL) and the reference capsule (C_max 2.4 ng/mL, AUC_0-72 11.7 h·ng/mL). The time to peak concentration (tmax) was shortest for the liquid (median ~ 1.0 h), followed by the capsule (2.0 h), and longest for the reference (6.0 h). Inter-individual variability in C_max and AUC was substantially lower for both novel formulations (coefficients of variation ~ 27-44%) than for the reference (> 90%). Statistical analysis confirmed that both the enhanced capsule and liquid produced significantly greater C_max and AUC_0-72 than the reference (geometric mean C_max ratios ~ 566% and ~ 248%, AUC_0-72 ratios ~ 328% and ~ 166%, respectively; 90% confidence intervals did not include 100%). The 7-hydroxy-CBD metabolite reached much lower plasma levels than parent CBD for all treatments (C_max 0.4-1.8 ng/mL, ~ 5-13% of parent C_max), with a slightly delayed tmax (~ 2-6 h) and similar elimination half-life. No serious AEs occurred. The only treatment-related AE was mild-to-moderate transient headache in four subjects (1 on capsule, 2 on liquid, 1 on reference), all resolved without intervention. No clinically significant changes in liver function tests or other laboratory values were observed. Plasma cortisol levels remained within normal ranges after all treatments, with a decline over 8 h consistent with the normal diurnal rhythm and no significant differences between formulations.</p><p><strong>Conclusions: </strong>Both novel formulations markedly improved CBD oral bioavailability under low-fat fed conditions relative to an unformulated CBD isolate capsule. The enhanced capsule in particular achieved a ~ 5.7-fold higher C_max and ~ 3.3-fold higher AUC than the reference, while the enhanced liquid was absorbed ~ 2.5-fold faster. Variability was reduced with the new formulations, and both were well tolerated at the 40 mg dose. These results indicate that the surfactant/acid formulation technology effectively enhances CBD absorption even with a low-fat meal, potentially obviating the need for high-fat co-administration. Further clinical studies (including in female subjects and at steady state) are warranted to confirm these pharmacokinetic advantages in broader populations.</p><p><strong>Trial registration: </strong>Not prospectively registered (pilot pharmacokinetic study without therapeutic intent, thus not subject to mandatory registration).</p>","PeriodicalId":101310,"journal":{"name":"Journal of cannabis research","volume":"7 1","pages":"54"},"PeriodicalIF":4.3000,"publicationDate":"2025-08-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12330118/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cannabis research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42238-025-00312-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study aimed to compare the pharmacokinetics and relative bioavailability of two novel cannabidiol (CBD) formulations including bioavailability-enhanced capsule (CBDNEXT Supra capsule) and a bioavailability-enhanced liquid (CBDNEXT Supra liquid)- against a standard high-purity CBD isolate capsule in healthy volunteers under fed (low-fat) conditions.
Methods: A single-dose, open-label, randomized, three-period, three-sequence crossover trial was conducted in 12 healthy male volunteers (18-50 years). Of the 12 enrolled subjects, 9 completed all three treatment periods per protocol. Each received 40 mg of CBD as one of three formulations: Test-1 (enhanced CBD capsule), Test-2 (enhanced CBD liquid), or Reference (unformulated CBD isolate capsule with microcrystalline cellulose only as excipient), with a washout of 14 days between treatments. All doses were administered 30 min after a standardized low-fat (~ 300-350 kcal, < 10 g fat) breakfast to minimize the impact of dietary fat on CBD absorption. Blood samples were collected up to 72 h post-dose for plasma CBD and 7-hydroxy-CBD analysis by a validated LC-MS/MS method (LLOQ 0.1 ng/mL). Pharmacokinetic (PK) parameters (C_max, tmax, AUC_0-72, and t_1/2) were determined by non-compartmental analysis. Safety was assessed by adverse events (AEs), vital signs, and laboratory tests (including liver enzymes). Plasma cortisol was measured pre-dose and at 2-, 4-, and 8-hours post-dose as an exploratory pharmacodynamic marker.
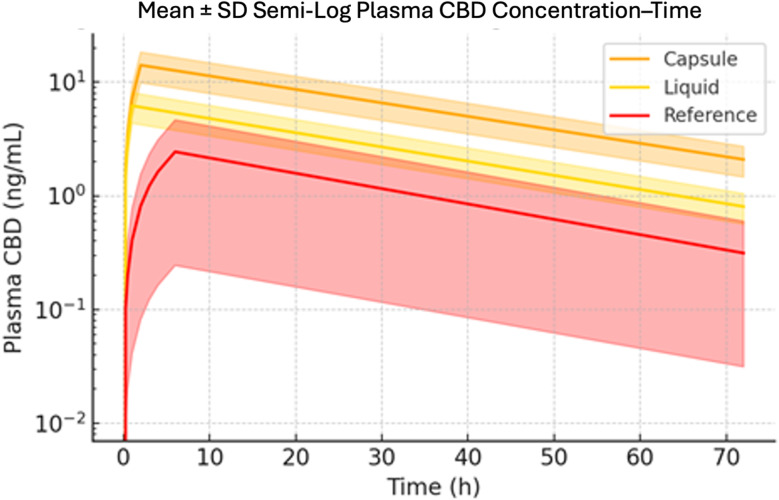
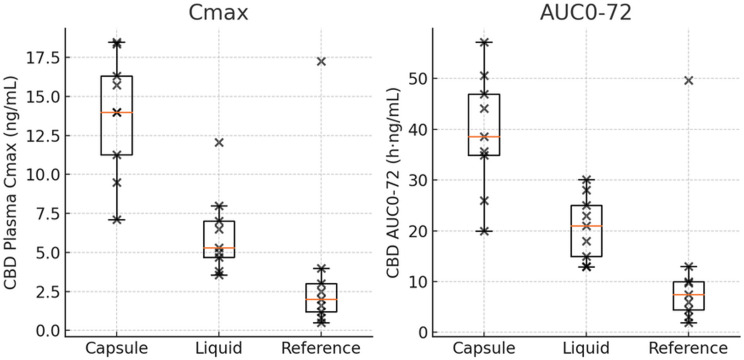
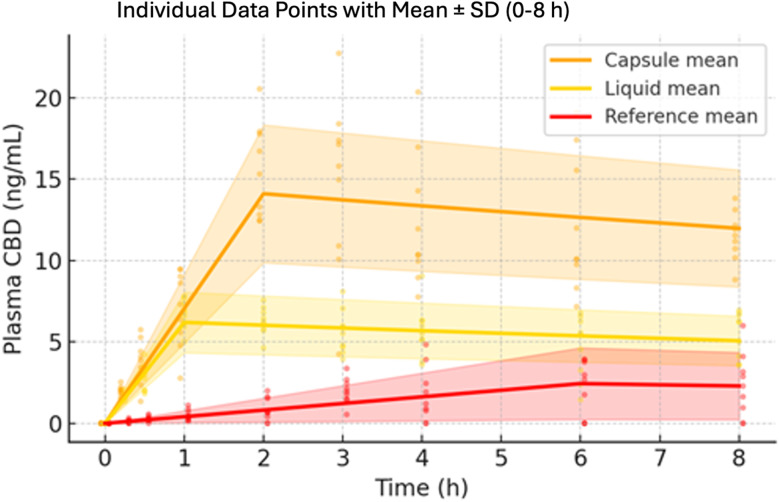
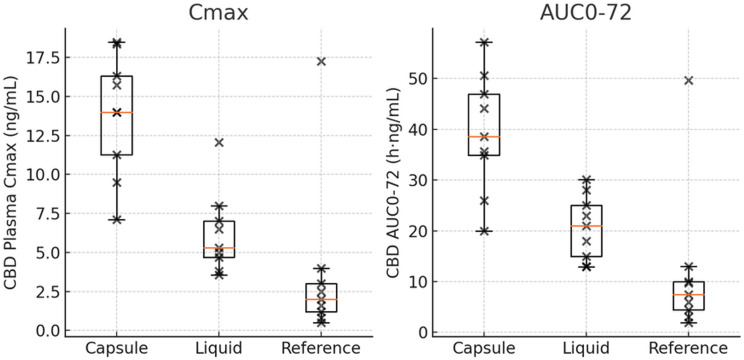
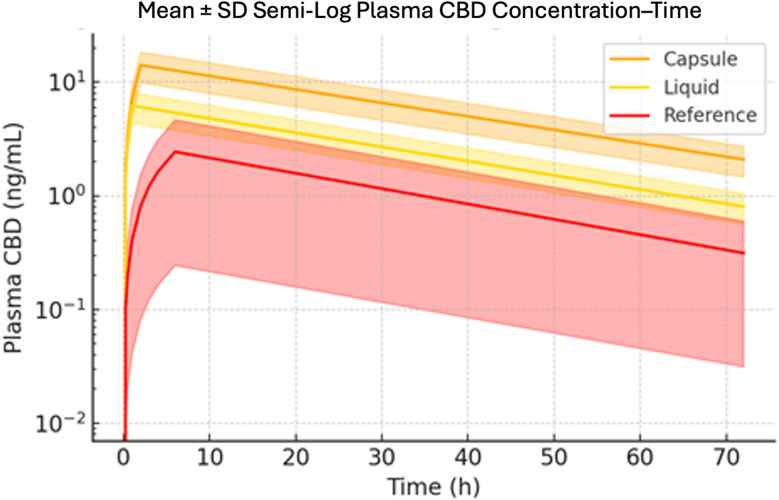
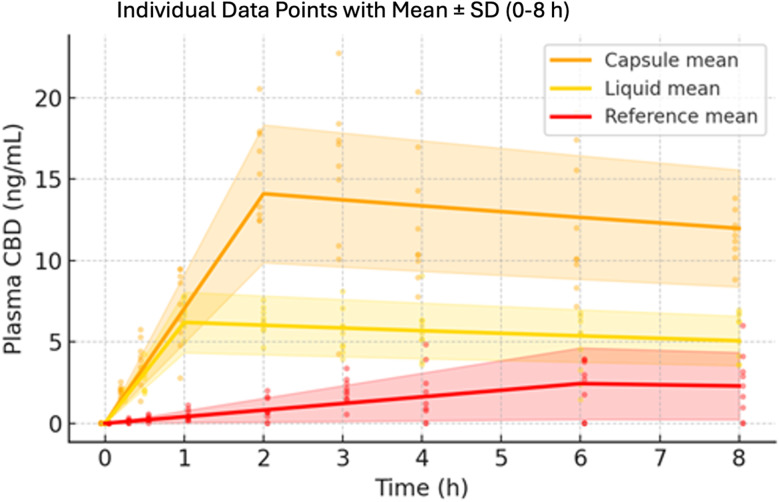
Results: Nine subjects completed all treatments (three withdrew: two for positive drug screens and one for an intercurrent moderate infection). Mean plasma CBD concentration-time profiles for the three formulations demonstrated markedly different absorption kinetics. The enhanced capsule achieved the highest peak CBD concentration (C_max 14.1 ng/mL) and exposure (AUC_0-72 38.0 h·ng/mL), compared to the enhanced liquid (C_max 6.2 ng/mL, AUC_0-72 20.2 h·ng/mL) and the reference capsule (C_max 2.4 ng/mL, AUC_0-72 11.7 h·ng/mL). The time to peak concentration (tmax) was shortest for the liquid (median ~ 1.0 h), followed by the capsule (2.0 h), and longest for the reference (6.0 h). Inter-individual variability in C_max and AUC was substantially lower for both novel formulations (coefficients of variation ~ 27-44%) than for the reference (> 90%). Statistical analysis confirmed that both the enhanced capsule and liquid produced significantly greater C_max and AUC_0-72 than the reference (geometric mean C_max ratios ~ 566% and ~ 248%, AUC_0-72 ratios ~ 328% and ~ 166%, respectively; 90% confidence intervals did not include 100%). The 7-hydroxy-CBD metabolite reached much lower plasma levels than parent CBD for all treatments (C_max 0.4-1.8 ng/mL, ~ 5-13% of parent C_max), with a slightly delayed tmax (~ 2-6 h) and similar elimination half-life. No serious AEs occurred. The only treatment-related AE was mild-to-moderate transient headache in four subjects (1 on capsule, 2 on liquid, 1 on reference), all resolved without intervention. No clinically significant changes in liver function tests or other laboratory values were observed. Plasma cortisol levels remained within normal ranges after all treatments, with a decline over 8 h consistent with the normal diurnal rhythm and no significant differences between formulations.
Conclusions: Both novel formulations markedly improved CBD oral bioavailability under low-fat fed conditions relative to an unformulated CBD isolate capsule. The enhanced capsule in particular achieved a ~ 5.7-fold higher C_max and ~ 3.3-fold higher AUC than the reference, while the enhanced liquid was absorbed ~ 2.5-fold faster. Variability was reduced with the new formulations, and both were well tolerated at the 40 mg dose. These results indicate that the surfactant/acid formulation technology effectively enhances CBD absorption even with a low-fat meal, potentially obviating the need for high-fat co-administration. Further clinical studies (including in female subjects and at steady state) are warranted to confirm these pharmacokinetic advantages in broader populations.
Trial registration: Not prospectively registered (pilot pharmacokinetic study without therapeutic intent, thus not subject to mandatory registration).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


