{"title":"Autoimmune enteropathy in adults: a case report and literature review.","authors":"Saifei Xu, Xiaotan Dou, Lei Wang, Chenggong Yu","doi":"10.21037/acr-25-24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Autoimmune enteropathy (AIE) is a rare autoimmune disorder characterized primarily by villous atrophy of the small intestinal mucosa. This article presents a case of adult-onset AIE featuring intractable diarrhea and severe malnutrition, along with a review of the existing literature to summarize its clinical characteristics, aiming to provide insights for the diagnosis and management of AIE.</p><p><strong>Case description: </strong>A 60-year-old male was admitted due to intermittent abdominal pain, diarrhea, and weight loss. Laboratory tests revealed gliadin immunoglobulin A (IgA) (+) and immunoglobulin G (IgG) (+), but tissue transglutaminase IgA (-) and IgG (-). Endoscopy revealed that the mucous membrane of the small intestine was congested and edematous, the villi were atrophied and prone to bleeding after biopsy, and some of the villi exhibited a white mossy appearance. Pathologically, the villi of many segments of the small intestine presented diffuse and obvious atrophy, and there was lymphocytic infiltration in the intestinal glands. After exclusionary diagnosis, the patient was considered to have AIE. After effective initial treatment with corticosteroid, the patient exhibited recurrent symptoms and poor nutritional status, and eventually died of sepsis.</p><p><strong>Conclusions: </strong>For patients with refractory diarrhea and intestinal villous atrophy, a comprehensive diagnosis should be made based on medication history, epidemiological factors, gluten dietary response, serological markers, and histopathological findings. Early intervention with corticosteroids combined with nutritional support is critical, while vigilance against severe adverse events such as life-threatening infections is essential.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"9 ","pages":"99"},"PeriodicalIF":0.7000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12319618/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-25-24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Autoimmune enteropathy (AIE) is a rare autoimmune disorder characterized primarily by villous atrophy of the small intestinal mucosa. This article presents a case of adult-onset AIE featuring intractable diarrhea and severe malnutrition, along with a review of the existing literature to summarize its clinical characteristics, aiming to provide insights for the diagnosis and management of AIE.
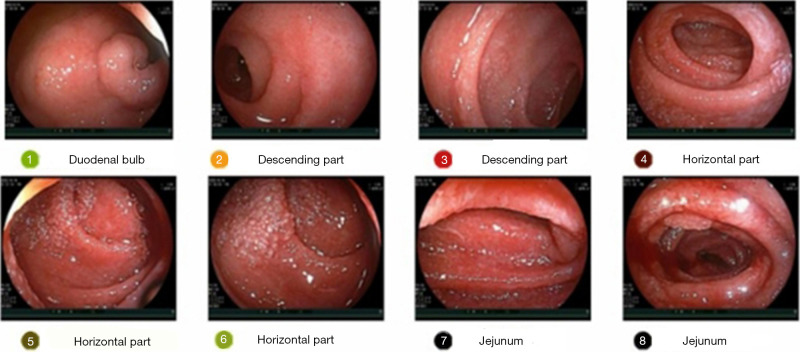
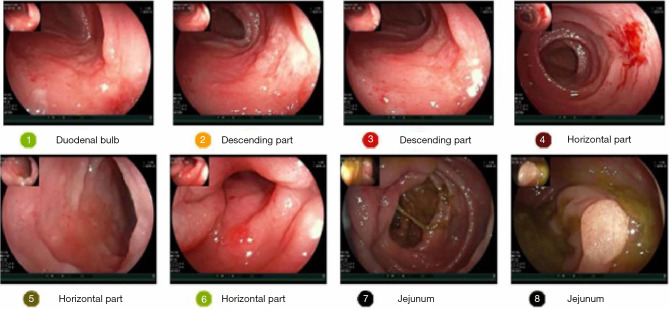
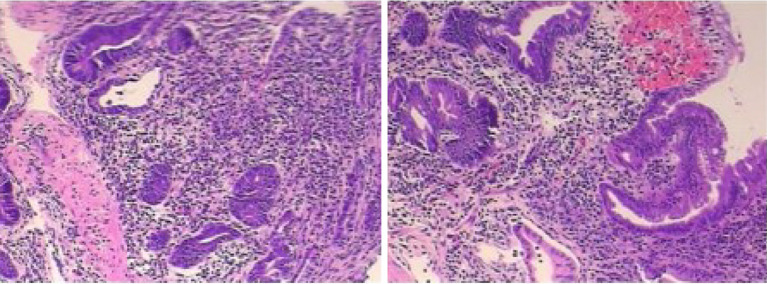
Case description: A 60-year-old male was admitted due to intermittent abdominal pain, diarrhea, and weight loss. Laboratory tests revealed gliadin immunoglobulin A (IgA) (+) and immunoglobulin G (IgG) (+), but tissue transglutaminase IgA (-) and IgG (-). Endoscopy revealed that the mucous membrane of the small intestine was congested and edematous, the villi were atrophied and prone to bleeding after biopsy, and some of the villi exhibited a white mossy appearance. Pathologically, the villi of many segments of the small intestine presented diffuse and obvious atrophy, and there was lymphocytic infiltration in the intestinal glands. After exclusionary diagnosis, the patient was considered to have AIE. After effective initial treatment with corticosteroid, the patient exhibited recurrent symptoms and poor nutritional status, and eventually died of sepsis.
Conclusions: For patients with refractory diarrhea and intestinal villous atrophy, a comprehensive diagnosis should be made based on medication history, epidemiological factors, gluten dietary response, serological markers, and histopathological findings. Early intervention with corticosteroids combined with nutritional support is critical, while vigilance against severe adverse events such as life-threatening infections is essential.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


