Som Singh, Sergio Abraham Candiales, Zachary Hunzeker, Cristina Olivo Freites, Modupe Idowu
{"title":"Thrombotic storm with antiphospholipid syndrome in the setting of relapsing Evans syndrome and systemic lupus erythematosus: a case report.","authors":"Som Singh, Sergio Abraham Candiales, Zachary Hunzeker, Cristina Olivo Freites, Modupe Idowu","doi":"10.21037/acr-24-190","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There are few cases that report the presence of lupus anticoagulant and antiphospholipid antibodies between Evans syndrome and the presence of lupus anticoagulant. However, differentiating between primary and secondary causes of Evans syndrome remains challenging.</p><p><strong>Case description: </strong>A 31-year-old female with a medical history of autism spectrum disorder, antiphospholipid syndrome (APS), complete systemic lupus erythematosus (SLE), and Evans syndrome was admitted for cholecystitis requiring laparoscopic cholecystectomy. In the setting of her acute illness, her thrombocytopenia worsened. Her hospital course was then complicated by the development of a left adrenal hematoma and venous thrombosis. Anticoagulation therapy was conservatively held due to concern for bleeding risk with the hematoma. However, given persistent thrombocytopenia, she subsequently underwent a platelet transfusion and was started on a 5-day course of intravenous immunoglobulin (IVIG). A venous Doppler ultrasound revealed a new occlusive deep venous thrombosis in the right axillary and brachial veins and occlusive venous thrombosis in the left cephalic veins while on the conservative anticoagulation regimen. This led to the immediate restart of anticoagulation therapy with close monitoring of coagulation labs. Her platelets improved Eltrombopag and IVIG up to 50,000 platelets/mcL.</p><p><strong>Conclusions: </strong>This case aims to highlight the challenges of managing thrombocytopenia in a patient with multiple autoimmune conditions on opposite ends of the coagulopathic spectrum in the inpatient setting.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"9 ","pages":"79"},"PeriodicalIF":0.7000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12319599/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-24-190","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There are few cases that report the presence of lupus anticoagulant and antiphospholipid antibodies between Evans syndrome and the presence of lupus anticoagulant. However, differentiating between primary and secondary causes of Evans syndrome remains challenging.
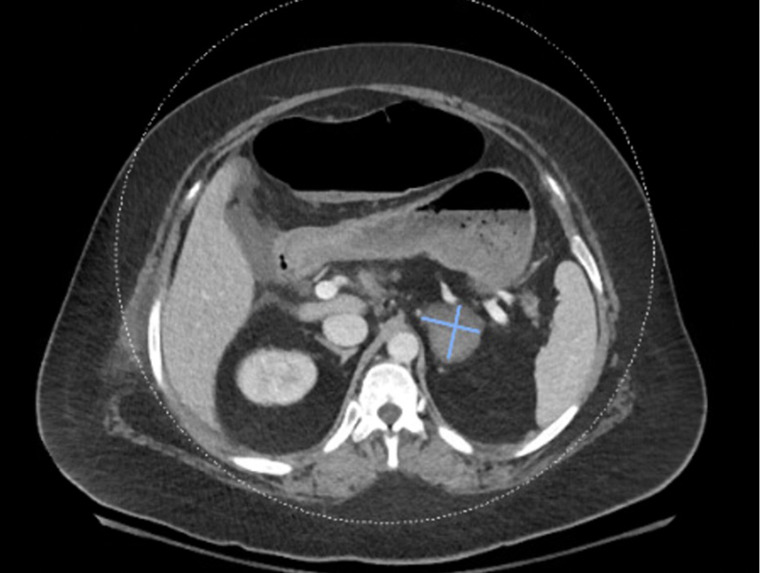
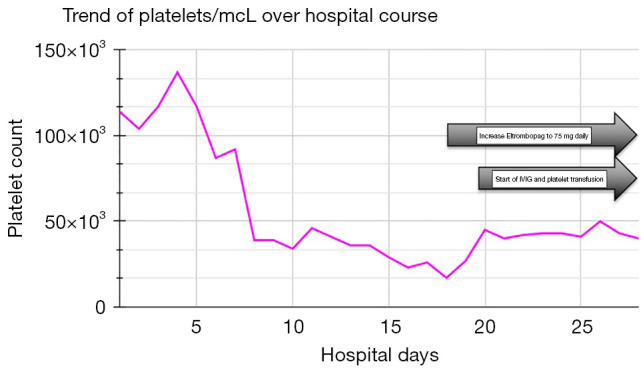
Case description: A 31-year-old female with a medical history of autism spectrum disorder, antiphospholipid syndrome (APS), complete systemic lupus erythematosus (SLE), and Evans syndrome was admitted for cholecystitis requiring laparoscopic cholecystectomy. In the setting of her acute illness, her thrombocytopenia worsened. Her hospital course was then complicated by the development of a left adrenal hematoma and venous thrombosis. Anticoagulation therapy was conservatively held due to concern for bleeding risk with the hematoma. However, given persistent thrombocytopenia, she subsequently underwent a platelet transfusion and was started on a 5-day course of intravenous immunoglobulin (IVIG). A venous Doppler ultrasound revealed a new occlusive deep venous thrombosis in the right axillary and brachial veins and occlusive venous thrombosis in the left cephalic veins while on the conservative anticoagulation regimen. This led to the immediate restart of anticoagulation therapy with close monitoring of coagulation labs. Her platelets improved Eltrombopag and IVIG up to 50,000 platelets/mcL.
Conclusions: This case aims to highlight the challenges of managing thrombocytopenia in a patient with multiple autoimmune conditions on opposite ends of the coagulopathic spectrum in the inpatient setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


