Abdul Rasheed Bahar, Fadi Kathawa, Tiffany Le, Abubaker Farah, Abdalaziz Awadelkarim, Hersimren Minhas, Luis Afonso
{"title":"Sinoatrial nodal reentrant tachycardia: a case report and literature review.","authors":"Abdul Rasheed Bahar, Fadi Kathawa, Tiffany Le, Abubaker Farah, Abdalaziz Awadelkarim, Hersimren Minhas, Luis Afonso","doi":"10.21037/acr-24-262","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sinoatrial nodal reentrant tachycardia (SANRT) is a rare form of focal atrial tachycardia, often linked with structural or congenital heart disease. Due to its electrocardiographic similarities with other supraventricular tachyarrhythmias, it is frequently misdiagnosed. Understanding its clinical presentation and effective management strategies is crucial for appropriate patient care.</p><p><strong>Case description: </strong>We present a case of a 45-year-old female with severe pulmonary hypertension and obstructive sleep apnea who was admitted with progressive palpitations, chest pain, and dyspnea. Initial electrocardiographic evaluation suggested atrial fibrillation with rapid ventricular response (RVR), leading to treatment with metoprolol and amiodarone. However, the tachyarrhythmia persisted, and further investigation revealed features suggestive of SANRT. The diagnosis was confirmed by telemetry findings demonstrating atrial tachycardia with a prolonged PR interval, terminating abruptly after carotid sinus massage (CSM). This immediate response to vagal stimulation solidified the diagnosis of SANRT. The patient was managed conservatively with vagal maneuver training and discharged on oral bisoprolol.</p><p><strong>Conclusions: </strong>This case highlights the diagnostic challenges associated with SANRT and emphasizes the role of CSM as both a diagnostic and therapeutic intervention. Early recognition of SANRT is crucial, as it can mimic other supraventricular arrhythmias, leading to mismanagement. While electrophysiological studies remain the gold standard for diagnosis, non-invasive measures such as vagal maneuvers can be highly effective in terminating the arrhythmia and providing symptomatic relief.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"9 ","pages":"80"},"PeriodicalIF":0.7000,"publicationDate":"2025-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12319621/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-24-262","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Sinoatrial nodal reentrant tachycardia (SANRT) is a rare form of focal atrial tachycardia, often linked with structural or congenital heart disease. Due to its electrocardiographic similarities with other supraventricular tachyarrhythmias, it is frequently misdiagnosed. Understanding its clinical presentation and effective management strategies is crucial for appropriate patient care.
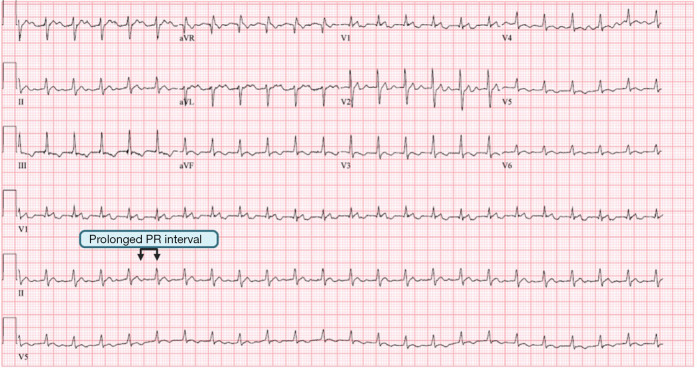
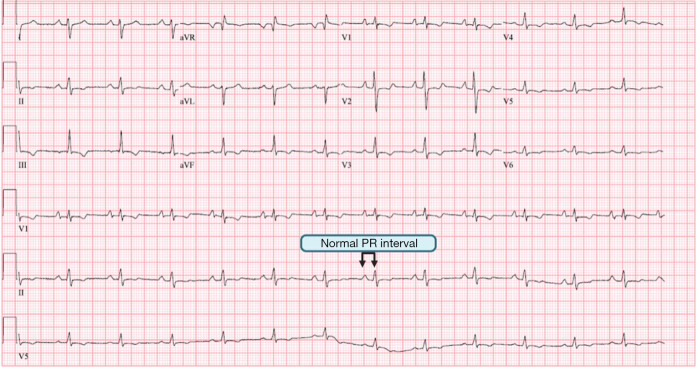
Case description: We present a case of a 45-year-old female with severe pulmonary hypertension and obstructive sleep apnea who was admitted with progressive palpitations, chest pain, and dyspnea. Initial electrocardiographic evaluation suggested atrial fibrillation with rapid ventricular response (RVR), leading to treatment with metoprolol and amiodarone. However, the tachyarrhythmia persisted, and further investigation revealed features suggestive of SANRT. The diagnosis was confirmed by telemetry findings demonstrating atrial tachycardia with a prolonged PR interval, terminating abruptly after carotid sinus massage (CSM). This immediate response to vagal stimulation solidified the diagnosis of SANRT. The patient was managed conservatively with vagal maneuver training and discharged on oral bisoprolol.
Conclusions: This case highlights the diagnostic challenges associated with SANRT and emphasizes the role of CSM as both a diagnostic and therapeutic intervention. Early recognition of SANRT is crucial, as it can mimic other supraventricular arrhythmias, leading to mismanagement. While electrophysiological studies remain the gold standard for diagnosis, non-invasive measures such as vagal maneuvers can be highly effective in terminating the arrhythmia and providing symptomatic relief.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


