Kacie Kerlee, Jasmina Ehab, Jeremy Watson, Patrick Weill, Raghav Chandra, Suresh Keshavamurthy, Ankeeta Mehta, Thomas H Shoultz
{"title":"Multifocal bowel perforation from angioinvasive aspergillosis after bilateral lung transplantation: a case report and review of the literature.","authors":"Kacie Kerlee, Jasmina Ehab, Jeremy Watson, Patrick Weill, Raghav Chandra, Suresh Keshavamurthy, Ankeeta Mehta, Thomas H Shoultz","doi":"10.21037/acr-24-221","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lung transplant recipients on immunosuppression are at increased risk for aggressive opportunistic infections, including invasive aspergillosis (IA). Distal septic embolization from angio-IA with involvement of the small and large bowel is extremely uncommon, and clinical manifestations of bowel ischemia and perforation may be masked due to immunosuppression.</p><p><strong>Case description: </strong>We present herein the first reported case of peritonitis secondary to jejunal and cecal perforation secondary to angio-IA after lung transplantation (LT) in a 62-year-old male. The patient was admitted to the hospital for acute cellular rejection requiring high-dose immunosuppression. His course was complicated by respiratory failure secondary to IA, with resulting multiorgan system dysfunction during which time peritonitis was noted on examination and cross-sectional imaging demonstrated pneumatosis, portal venous gas, and pneumoperitoneum. The patient required emergent surgical intervention and underwent an exploratory laparotomy, jejunal resection, right hemicolectomy, and end ileostomy with colonic mucus fistula. Final pathologic analysis of resected specimens demonstrated angio-IA in both the jejunal and cecal segments with associated transmural ischemic necrosis.</p><p><strong>Conclusions: </strong>Bowel perforation secondary to angio-IA is a very rare but serious complication after LT that is associated with high morbidity and mortality. Evaluation requires a high index of suspicion in the setting of immunosuppression and often concomitant extraintestinal pathologies. Early, aggressive surgical intervention is necessary.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"9 ","pages":"91"},"PeriodicalIF":0.7000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12319623/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-24-221","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Lung transplant recipients on immunosuppression are at increased risk for aggressive opportunistic infections, including invasive aspergillosis (IA). Distal septic embolization from angio-IA with involvement of the small and large bowel is extremely uncommon, and clinical manifestations of bowel ischemia and perforation may be masked due to immunosuppression.
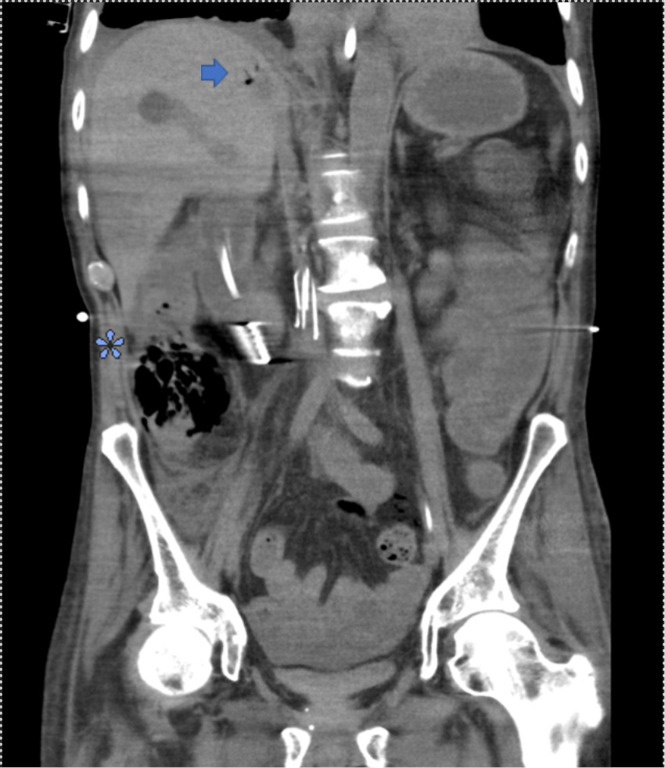
Case description: We present herein the first reported case of peritonitis secondary to jejunal and cecal perforation secondary to angio-IA after lung transplantation (LT) in a 62-year-old male. The patient was admitted to the hospital for acute cellular rejection requiring high-dose immunosuppression. His course was complicated by respiratory failure secondary to IA, with resulting multiorgan system dysfunction during which time peritonitis was noted on examination and cross-sectional imaging demonstrated pneumatosis, portal venous gas, and pneumoperitoneum. The patient required emergent surgical intervention and underwent an exploratory laparotomy, jejunal resection, right hemicolectomy, and end ileostomy with colonic mucus fistula. Final pathologic analysis of resected specimens demonstrated angio-IA in both the jejunal and cecal segments with associated transmural ischemic necrosis.
Conclusions: Bowel perforation secondary to angio-IA is a very rare but serious complication after LT that is associated with high morbidity and mortality. Evaluation requires a high index of suspicion in the setting of immunosuppression and often concomitant extraintestinal pathologies. Early, aggressive surgical intervention is necessary.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


