Mortality and Graft Failure With Medical Management Alone Versus Revascularization After Coronary Angiography Among Kidney Transplant Recipients: A Population-Based Study.
Labib I Faruque, Robert R Quinn, Pietro Ravani, Tyrone G Harrison, Brenda Hemmelgarn, Stephen Wilton, Alix Clarke, Matthew T James, Ngan N Lam
{"title":"Mortality and Graft Failure With Medical Management Alone Versus Revascularization After Coronary Angiography Among Kidney Transplant Recipients: A Population-Based Study.","authors":"Labib I Faruque, Robert R Quinn, Pietro Ravani, Tyrone G Harrison, Brenda Hemmelgarn, Stephen Wilton, Alix Clarke, Matthew T James, Ngan N Lam","doi":"10.1177/20543581251358143","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There are limited data on the outcomes following medical management alone versus revascularization (percutaneous coronary intervention [PCI] or coronary artery bypass grafting [CABG]) after coronary angiography in kidney transplant recipients.</p><p><strong>Objective: </strong>The objective was to compare survival and graft loss in kidney transplant recipients treated with medical therapy alone versus coronary revascularization following coronary angiography.</p><p><strong>Design: </strong>We conducted a retrospective, population-based cohort study using linked health care databases.</p><p><strong>Setting: </strong>This study was conducted in Alberta, Canada.</p><p><strong>Patients: </strong>We included adult, kidney-only transplant recipients between January 1997 and March 2015 who survived at least 1-year post-transplant with a functioning graft and had a coronary angiography during follow-up.</p><p><strong>Measurements: </strong>The outcomes were all-cause mortality, death-censored graft failure, death with a functioning graft, and all-cause graft failure.</p><p><strong>Methods: </strong>We ascertained baseline characteristics, covariate information, and outcome data from the Alberta Kidney Disease Network (AKDN) and Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease (APPROACH) databases. We used Cox proportional hazards models to compare mortality and graft loss between recipients treated with medical management versus revascularization (PCI or CABG) following angiography.</p><p><strong>Results: </strong>We identified 142 kidney transplant recipients who received a coronary angiography: 69 (49%) were treated with medical management, and 73 (51%) were treated with revascularization (PCI n = 52, CABG n = 21). The median age was 60 years (interquartile range [IQR] 50-66), 76% were male, the median baseline estimated glomerular filtration rate (eGFR) was 54 mL/min/1.73 m<sup>2</sup> (IQR 41-69), and the median follow-up was 5 years (IQR 2-8). Compared to medical management, recipients treated with revascularization did not have statistically higher risk of all-cause mortality (55% vs 62%; 80 vs 102 events/1000 person-years; adjusted hazard ratio [aHR] 1.32, 95% CI 0.86-2.02; <i>P</i> = .21). There was no significant difference in death-censored graft failure between the two treatment groups (20% vs 22%; 33 vs 40 events/1000 person-years; aHR 1.22, 95% CI 0.58-2.58; <i>P</i> = .60).</p><p><strong>Limitations: </strong>The clinical indications for medical management alone versus revascularization might influence the choice of these interventions. Due to the smaller sample size, we could not present the outcomes by PCI versus CABG. We also did not have complete data on blood pressure, body mass index, or medication usage which might have influenced our outcomes.</p><p><strong>Conclusions: </strong>In kidney transplant recipients undergoing coronary angiography, the rate of mortality was more than double that of graft failure, regardless of post-angiography management of coronary artery disease. The high overall risk for both groups requires further exploration in larger cohorts with longer follow-up.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251358143"},"PeriodicalIF":1.5000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12319199/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251358143","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There are limited data on the outcomes following medical management alone versus revascularization (percutaneous coronary intervention [PCI] or coronary artery bypass grafting [CABG]) after coronary angiography in kidney transplant recipients.
Objective: The objective was to compare survival and graft loss in kidney transplant recipients treated with medical therapy alone versus coronary revascularization following coronary angiography.
Design: We conducted a retrospective, population-based cohort study using linked health care databases.
Setting: This study was conducted in Alberta, Canada.
Patients: We included adult, kidney-only transplant recipients between January 1997 and March 2015 who survived at least 1-year post-transplant with a functioning graft and had a coronary angiography during follow-up.
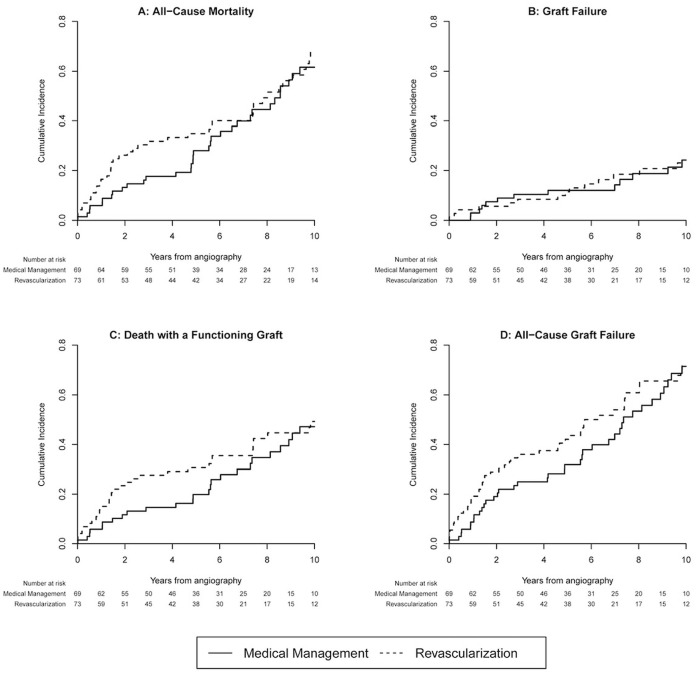
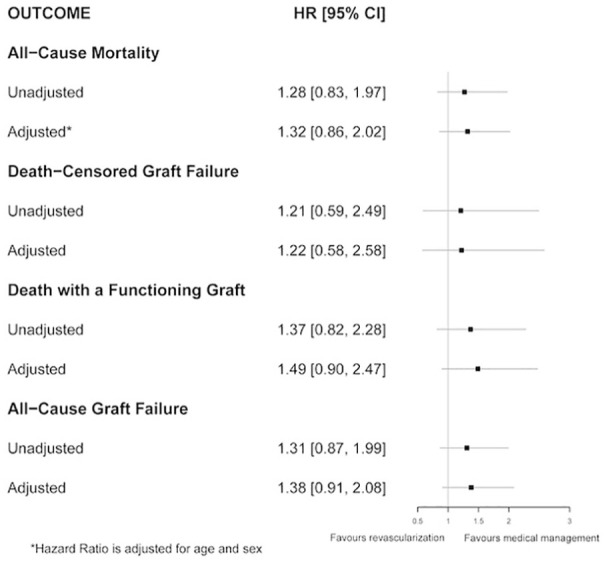
Measurements: The outcomes were all-cause mortality, death-censored graft failure, death with a functioning graft, and all-cause graft failure.
Methods: We ascertained baseline characteristics, covariate information, and outcome data from the Alberta Kidney Disease Network (AKDN) and Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease (APPROACH) databases. We used Cox proportional hazards models to compare mortality and graft loss between recipients treated with medical management versus revascularization (PCI or CABG) following angiography.
Results: We identified 142 kidney transplant recipients who received a coronary angiography: 69 (49%) were treated with medical management, and 73 (51%) were treated with revascularization (PCI n = 52, CABG n = 21). The median age was 60 years (interquartile range [IQR] 50-66), 76% were male, the median baseline estimated glomerular filtration rate (eGFR) was 54 mL/min/1.73 m2 (IQR 41-69), and the median follow-up was 5 years (IQR 2-8). Compared to medical management, recipients treated with revascularization did not have statistically higher risk of all-cause mortality (55% vs 62%; 80 vs 102 events/1000 person-years; adjusted hazard ratio [aHR] 1.32, 95% CI 0.86-2.02; P = .21). There was no significant difference in death-censored graft failure between the two treatment groups (20% vs 22%; 33 vs 40 events/1000 person-years; aHR 1.22, 95% CI 0.58-2.58; P = .60).
Limitations: The clinical indications for medical management alone versus revascularization might influence the choice of these interventions. Due to the smaller sample size, we could not present the outcomes by PCI versus CABG. We also did not have complete data on blood pressure, body mass index, or medication usage which might have influenced our outcomes.
Conclusions: In kidney transplant recipients undergoing coronary angiography, the rate of mortality was more than double that of graft failure, regardless of post-angiography management of coronary artery disease. The high overall risk for both groups requires further exploration in larger cohorts with longer follow-up.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


