The contribution of minimally invasive tissue sampling compared to antemortem-derived cause of death determination among inpatient child deaths: the minimally invasive tissue sampling in Malawi study.
IF 4.3 3区 医学Q1 PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH
Wieger P Voskuijl, Dennis Chasweka, Sarah Lawrence, Daniella Brals, Steve Kamiza, Robert Bandsma, James A Berkley, Emmie Mbale, Charalampos Attipa, Chisomo Eneya, Cornelius Huwa, Stanley Khoswe, Christopher Moxon, Isabel Potani, Jessica L Waller, Maureen H Diaz, Judd Walson, Jaume Ordi, Donna M Denno
{"title":"The contribution of minimally invasive tissue sampling compared to antemortem-derived cause of death determination among inpatient child deaths: the minimally invasive tissue sampling in Malawi study.","authors":"Wieger P Voskuijl, Dennis Chasweka, Sarah Lawrence, Daniella Brals, Steve Kamiza, Robert Bandsma, James A Berkley, Emmie Mbale, Charalampos Attipa, Chisomo Eneya, Cornelius Huwa, Stanley Khoswe, Christopher Moxon, Isabel Potani, Jessica L Waller, Maureen H Diaz, Judd Walson, Jaume Ordi, Donna M Denno","doi":"10.7189/jogh.15.04210","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Improved causes of death (CoD) understanding in low- and middle-income countries is needed to reduce child mortality. Compared to full autopsy, minimally invasive tissue sampling (MITS), using transcutaneous needle sampling, is a feasible, socially acceptable, and validated method. We aimed to quantify the additional contribution of MITS to CoD attribution based on clinical records and inpatient research data with intensive patient characterisation.</p><p><strong>Methods: </strong>We enrolled children aged seven days to 59 months who died while on admission for acute illness and/or severe malnutrition to Queen Elizabeth Central Hospital in Blantyre, Malawi. Standard MITS procedures included histologic, immunohistochemical, and microbiologic testing. Phase 1 CoD determination was based on medical records alone, Phase 2 also included research data, and Phase 3 included all data, including from MITS.</p><p><strong>Results: </strong>We enrolled 29 children. Based on clinical notes alone (Phase 1), we identified 60 causal and 39 contributing conditions. Of the 45 (45%) infectious conditions, pathogens were identified in 15 (33%). Only one patient's (3%) CoD was unchanged compared to including all data (Phase 3). Further, we identified 69 new (n = 43) or adjusted (n = 26) diagnoses among 28 cases (97%); the majority were undernutrition-related (n = 22, 32%) or infectious (n = 41, 59%) conditions. Overall, the majority of final Phase 3 conditions were also undernutrition-related (n = 46, 32%) or infectious (n = 61, 43%) and a pathogen was identified in 54 (89%) of the infectious conditions. Klebsiella pneumoniae was the most prevalent aetiology in both pneumonia and sepsis.</p><p><strong>Conclusions: </strong>The addition of MITS to clinical and inpatient research data led to almost all (97%) of cases receiving new and/or refined diagnoses, including microbe identification in infectious conditions. Pathogens not specifically addressed by current clinical guidelines, such as Klebisiella pneumoniae, were commonly identified. Our findings support the utility of MITS to understand CoD even after thorough clinical characterisation of children during hospitalisation.</p>","PeriodicalId":48734,"journal":{"name":"Journal of Global Health","volume":"15 ","pages":"04210"},"PeriodicalIF":4.3000,"publicationDate":"2025-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12319396/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Global Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.7189/jogh.15.04210","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Improved causes of death (CoD) understanding in low- and middle-income countries is needed to reduce child mortality. Compared to full autopsy, minimally invasive tissue sampling (MITS), using transcutaneous needle sampling, is a feasible, socially acceptable, and validated method. We aimed to quantify the additional contribution of MITS to CoD attribution based on clinical records and inpatient research data with intensive patient characterisation.
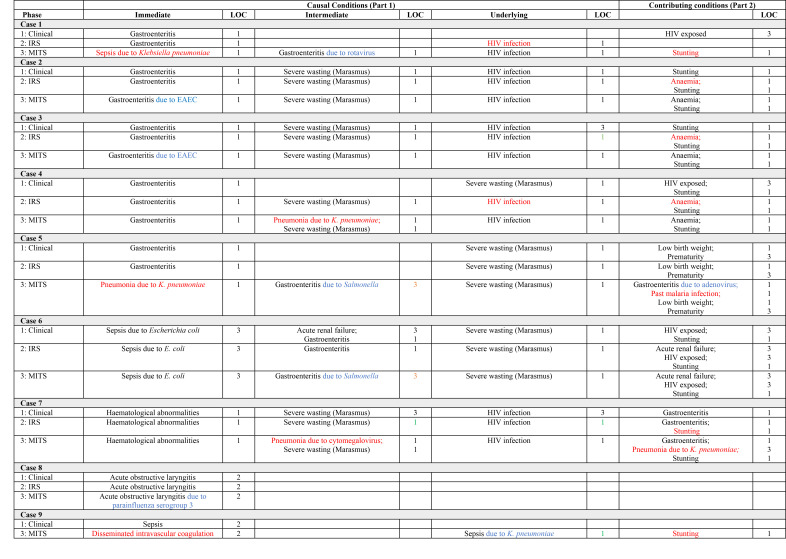
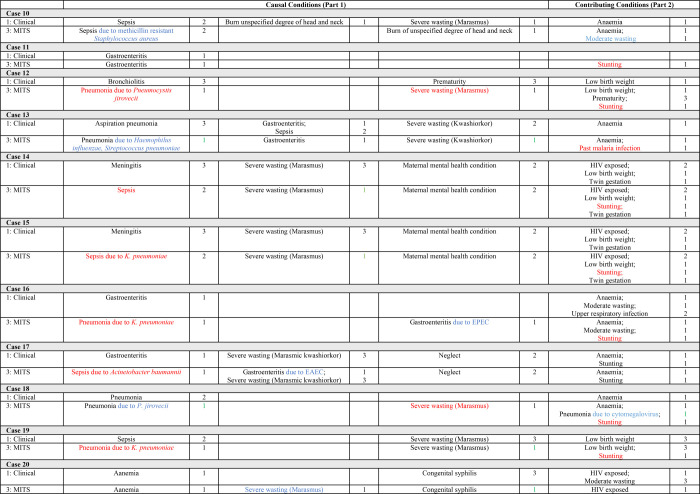
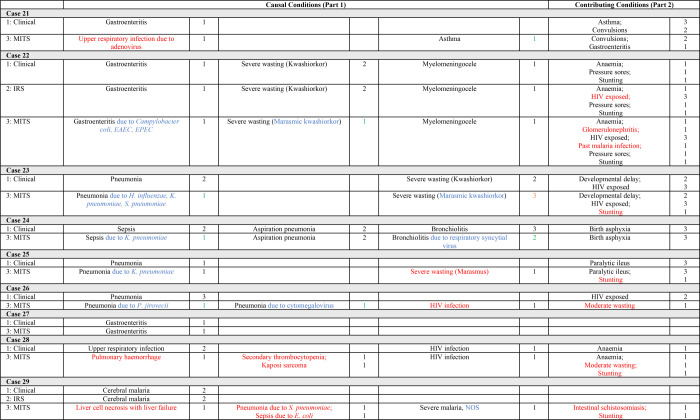
Methods: We enrolled children aged seven days to 59 months who died while on admission for acute illness and/or severe malnutrition to Queen Elizabeth Central Hospital in Blantyre, Malawi. Standard MITS procedures included histologic, immunohistochemical, and microbiologic testing. Phase 1 CoD determination was based on medical records alone, Phase 2 also included research data, and Phase 3 included all data, including from MITS.
Results: We enrolled 29 children. Based on clinical notes alone (Phase 1), we identified 60 causal and 39 contributing conditions. Of the 45 (45%) infectious conditions, pathogens were identified in 15 (33%). Only one patient's (3%) CoD was unchanged compared to including all data (Phase 3). Further, we identified 69 new (n = 43) or adjusted (n = 26) diagnoses among 28 cases (97%); the majority were undernutrition-related (n = 22, 32%) or infectious (n = 41, 59%) conditions. Overall, the majority of final Phase 3 conditions were also undernutrition-related (n = 46, 32%) or infectious (n = 61, 43%) and a pathogen was identified in 54 (89%) of the infectious conditions. Klebsiella pneumoniae was the most prevalent aetiology in both pneumonia and sepsis.
Conclusions: The addition of MITS to clinical and inpatient research data led to almost all (97%) of cases receiving new and/or refined diagnoses, including microbe identification in infectious conditions. Pathogens not specifically addressed by current clinical guidelines, such as Klebisiella pneumoniae, were commonly identified. Our findings support the utility of MITS to understand CoD even after thorough clinical characterisation of children during hospitalisation.
期刊介绍:
Journal of Global Health is a peer-reviewed journal published by the Edinburgh University Global Health Society, a not-for-profit organization registered in the UK. We publish editorials, news, viewpoints, original research and review articles in two issues per year.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


