Adina Landsberg, Nicole K Brockman, Emir Sevinc, Caitlin McClurg, Meghan J Elliott, Louis-Philippe Girard, Matthew T James, Alexander A Leung, Neesh I Pannu, Meghann Pasternak, Paul E Ronksley, Marcello Tonelli, Tyrone G Harrison
{"title":"Interventions to Reduce the Risk of Hypocalcemia After Parathyroidectomy for People With Advanced Chronic Kidney Disease: A Systematic Review.","authors":"Adina Landsberg, Nicole K Brockman, Emir Sevinc, Caitlin McClurg, Meghan J Elliott, Louis-Philippe Girard, Matthew T James, Alexander A Leung, Neesh I Pannu, Meghann Pasternak, Paul E Ronksley, Marcello Tonelli, Tyrone G Harrison","doi":"10.1177/20543581251358144","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>People with advanced chronic kidney disease (CKD) and secondary hyperparathyroidism (sHPT) refractory to medical therapy often require surgical parathyroidectomy. Severe and prolonged hypocalcemia immediately following parathyroidectomy for sHPT is often termed \"hungry bone syndrome\" (HBS).</p><p><strong>Objective: </strong>To systematically review the effect of pre-operative interventions on post-operative hypocalcemia, HBS, and other related outcomes in patients with CKD and sHPT undergoing parathyroidectomy.</p><p><strong>Design: </strong>This is a systematic review study.</p><p><strong>Setting: </strong>Diverse study designs conducted in any country.</p><p><strong>Patients: </strong>Adult patients with CKD complicated by sHPT undergoing parathyroidectomy.</p><p><strong>Measurements: </strong>Post-operative hypocalcemia, HBS, symptomatic hypocalcemia, and other related outcomes.</p><p><strong>Methods: </strong>We searched Ovid MEDLINE, Embase, and Cochrane Controlled Trials Registry from inception until June 2024 for trials and observational studies of adults with CKD and sHPT that evaluated pre-operative interventions aimed at reducing the risk of hypocalcemia following parathyroidectomy. After 2 phases of study screening conducted in duplicate, we extracted data on study design, patient characteristics, interventions, and outcomes. Hypocalcemia was defined as serum calcium <2.1 mmol/L and HBS as calcium <2.1 mmol/L for ≥4 days post-operatively. We evaluated the risk of bias and completed a narrative synthesis of the available literature across intervention types.</p><p><strong>Results: </strong>We identified 3616 studies; 35 underwent full-text review, and 9 met final eligibility criteria. Interventions included pre-operative calcitriol (n = 2), pre-operative cinacalcet (n = 3), pre-operative alkaline phosphatase (ALP) measurement to guide intravenous (IV) calcium administration (n = 3), and pre-operative pamidronate (n = 1). All studies reported on at least one of: median/mean post-operative calcium (n = 7), incidence of post-operative hypocalcemia (n = 3), HBS (n = 1), and symptomatic hypocalcemia (n = 4). Interventions that reported on the risk of post-operative hypocalcemia included pre-operative pamidronate (n = 1, 37 participants, odds ratio [OR] = 0.003, 95% confidence interval [CI] = 0.000-0.072) and IV calcium guided by pre-operative ALP (n = 1, 271 participants, OR = 0.292, 95% CI = 0.175-0.488). There were insufficient data to meta-analyze study-specific effects for any intervention or outcome.</p><p><strong>Limitations: </strong>Our study was limited by significant heterogeneity in outcome reporting, which resulted in substantial outcome reporting bias and prevented pooled analyses. Furthermore, no randomized control trials met our inclusion criteria, which limited assessment of publication bias.</p><p><strong>Conclusions: </strong>Pre-operative risk factors for HBS have been established in patients with CKD undergoing parathyroidectomy. However, limited research has evaluated pre-operative interventions to reduce the risk of HBS, and due to heterogeneity in outcome reporting across studies, there is still uncertainty about the effectiveness of such interventions. These findings support the need for future clinical trials.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251358144"},"PeriodicalIF":1.5000,"publicationDate":"2025-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12314243/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251358144","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: People with advanced chronic kidney disease (CKD) and secondary hyperparathyroidism (sHPT) refractory to medical therapy often require surgical parathyroidectomy. Severe and prolonged hypocalcemia immediately following parathyroidectomy for sHPT is often termed "hungry bone syndrome" (HBS).
Objective: To systematically review the effect of pre-operative interventions on post-operative hypocalcemia, HBS, and other related outcomes in patients with CKD and sHPT undergoing parathyroidectomy.
Design: This is a systematic review study.
Setting: Diverse study designs conducted in any country.
Patients: Adult patients with CKD complicated by sHPT undergoing parathyroidectomy.
Measurements: Post-operative hypocalcemia, HBS, symptomatic hypocalcemia, and other related outcomes.
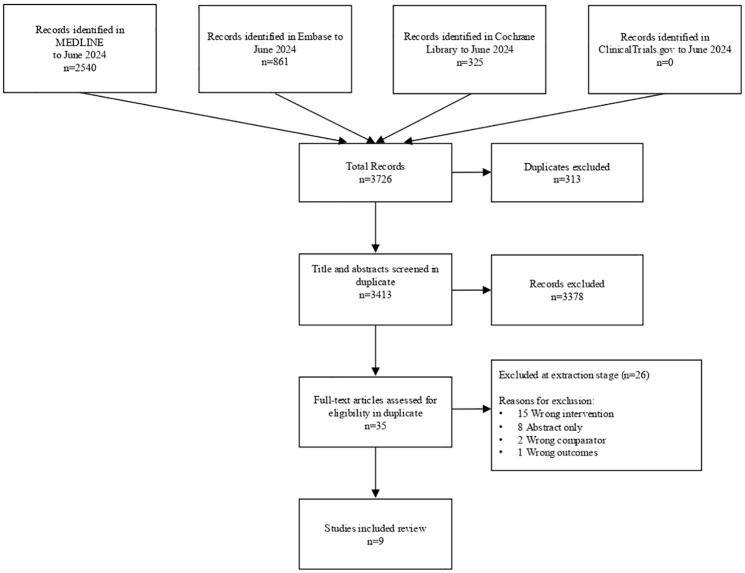
Methods: We searched Ovid MEDLINE, Embase, and Cochrane Controlled Trials Registry from inception until June 2024 for trials and observational studies of adults with CKD and sHPT that evaluated pre-operative interventions aimed at reducing the risk of hypocalcemia following parathyroidectomy. After 2 phases of study screening conducted in duplicate, we extracted data on study design, patient characteristics, interventions, and outcomes. Hypocalcemia was defined as serum calcium <2.1 mmol/L and HBS as calcium <2.1 mmol/L for ≥4 days post-operatively. We evaluated the risk of bias and completed a narrative synthesis of the available literature across intervention types.
Results: We identified 3616 studies; 35 underwent full-text review, and 9 met final eligibility criteria. Interventions included pre-operative calcitriol (n = 2), pre-operative cinacalcet (n = 3), pre-operative alkaline phosphatase (ALP) measurement to guide intravenous (IV) calcium administration (n = 3), and pre-operative pamidronate (n = 1). All studies reported on at least one of: median/mean post-operative calcium (n = 7), incidence of post-operative hypocalcemia (n = 3), HBS (n = 1), and symptomatic hypocalcemia (n = 4). Interventions that reported on the risk of post-operative hypocalcemia included pre-operative pamidronate (n = 1, 37 participants, odds ratio [OR] = 0.003, 95% confidence interval [CI] = 0.000-0.072) and IV calcium guided by pre-operative ALP (n = 1, 271 participants, OR = 0.292, 95% CI = 0.175-0.488). There were insufficient data to meta-analyze study-specific effects for any intervention or outcome.
Limitations: Our study was limited by significant heterogeneity in outcome reporting, which resulted in substantial outcome reporting bias and prevented pooled analyses. Furthermore, no randomized control trials met our inclusion criteria, which limited assessment of publication bias.
Conclusions: Pre-operative risk factors for HBS have been established in patients with CKD undergoing parathyroidectomy. However, limited research has evaluated pre-operative interventions to reduce the risk of HBS, and due to heterogeneity in outcome reporting across studies, there is still uncertainty about the effectiveness of such interventions. These findings support the need for future clinical trials.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


