Alberto Giuseppe Agostara, Sara Di Bella, Laura Bosotti, Michela Pelliccione, Paola Candido, Valeria Smiroldo, Silvia Della Torre, Giuseppe De Angelis, Roberto Bollina
{"title":"Kounis Syndrome Induced by Atezolizumab in a Patient with Non-Small Cell Lung Cancer: A Case Report.","authors":"Alberto Giuseppe Agostara, Sara Di Bella, Laura Bosotti, Michela Pelliccione, Paola Candido, Valeria Smiroldo, Silvia Della Torre, Giuseppe De Angelis, Roberto Bollina","doi":"10.1159/000546352","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Kounis syndrome (KS) is a rare and often underdiagnosed condition characterized by acute coronary syndromes triggered by allergic or anaphylactic reactions. This syndrome is particularly relevant in the context of immunotherapy, where immune checkpoint inhibitors (ICIs) such as atezolizumab are increasingly used in the treatment of advanced cancers. While atezolizumab is generally well-tolerated, immune-related adverse events, including cardiovascular toxicity, have been reported. Understanding the potential for ICIs to induce severe complications like KS is essential for ensuring patient safety and effective management.</p><p><strong>Case presentation: </strong>A smoker in their 70s with metastatic lung adenocarcinoma experienced an anaphylactic reaction during the second cycle of atezolizumab. The reaction was accompanied by chest tightness and elevated troponin T levels. Echocardiographic evaluation revealed severe dilatation of the left ventricular apex and a significantly reduced left ventricular ejection fraction. Coronary angiography excluded significant coronary stenosis but confirmed apical ballooning, consistent with the type I variant of KS. This diagnosis underscores the potential for immune-related cardiovascular events associated with ICIs to mimic acute coronary syndromes, challenging clinicians to distinguish between immune-mediated effects and primary cardiac conditions.</p><p><strong>Conclusions: </strong>This case highlights the importance of recognizing KS as a potential differential diagnosis in patients undergoing immunotherapy who present with acute coronary symptoms. The findings suggest that atezolizumab may trigger severe immune-related cardiovascular toxicity, emphasizing the need for vigilance among clinicians. Further research is warranted to elucidate the mechanisms linking ICIs to KS and to develop effective management and preventive strategies. Early recognition and prompt intervention are critical to mitigating risks and improving outcomes for patients receiving ICIs.</p>","PeriodicalId":9625,"journal":{"name":"Case Reports in Oncology","volume":"18 1","pages":"1034-1039"},"PeriodicalIF":0.7000,"publicationDate":"2025-07-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12316447/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000546352","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Kounis syndrome (KS) is a rare and often underdiagnosed condition characterized by acute coronary syndromes triggered by allergic or anaphylactic reactions. This syndrome is particularly relevant in the context of immunotherapy, where immune checkpoint inhibitors (ICIs) such as atezolizumab are increasingly used in the treatment of advanced cancers. While atezolizumab is generally well-tolerated, immune-related adverse events, including cardiovascular toxicity, have been reported. Understanding the potential for ICIs to induce severe complications like KS is essential for ensuring patient safety and effective management.
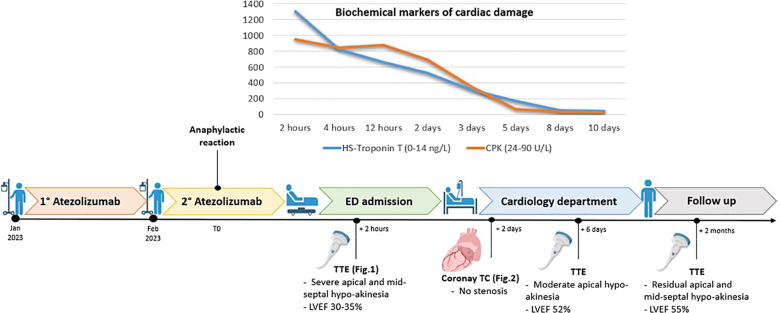
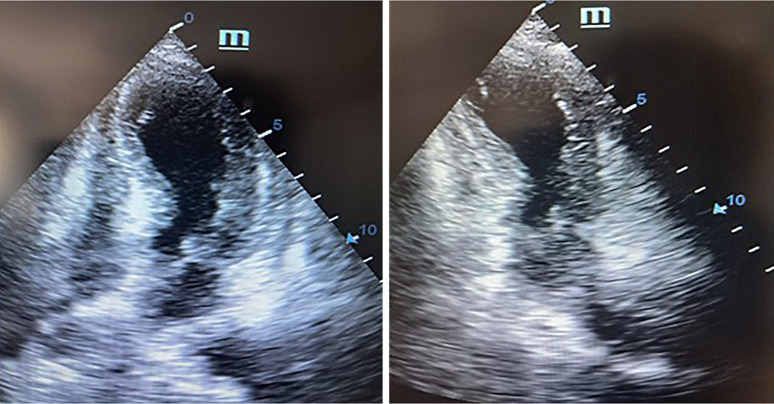
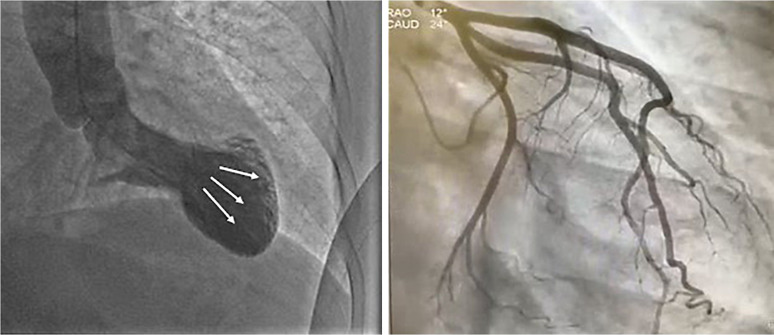
Case presentation: A smoker in their 70s with metastatic lung adenocarcinoma experienced an anaphylactic reaction during the second cycle of atezolizumab. The reaction was accompanied by chest tightness and elevated troponin T levels. Echocardiographic evaluation revealed severe dilatation of the left ventricular apex and a significantly reduced left ventricular ejection fraction. Coronary angiography excluded significant coronary stenosis but confirmed apical ballooning, consistent with the type I variant of KS. This diagnosis underscores the potential for immune-related cardiovascular events associated with ICIs to mimic acute coronary syndromes, challenging clinicians to distinguish between immune-mediated effects and primary cardiac conditions.
Conclusions: This case highlights the importance of recognizing KS as a potential differential diagnosis in patients undergoing immunotherapy who present with acute coronary symptoms. The findings suggest that atezolizumab may trigger severe immune-related cardiovascular toxicity, emphasizing the need for vigilance among clinicians. Further research is warranted to elucidate the mechanisms linking ICIs to KS and to develop effective management and preventive strategies. Early recognition and prompt intervention are critical to mitigating risks and improving outcomes for patients receiving ICIs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


