Impacts of mandatory clinical ethics consultation on resource utilization and ethical conflicts in critically ill patients: a comparison between medical and surgical intensive care units.
{"title":"Impacts of mandatory clinical ethics consultation on resource utilization and ethical conflicts in critically ill patients: a comparison between medical and surgical intensive care units.","authors":"Yen-Ko Lin, Chao-Wen Chen, Yung-Sung Yeh, Chia-Ju Lin, Yu-Wen Huang, Yu-Chih Lin, Chau-Chyun Sheu","doi":"10.1186/s12910-025-01268-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Mandatory clinical ethics consultation (CEC) is initiated under specific circumstances when required by institutional policies. Medical and surgical intensive care units (ICUs) have various characteristics. Studies on whether mandatory CEC have different impacts on medical and surgical ICUs are limited. This study aimed to investigate the impacts of mandatory CEC on resource use and ethical conflicts as well as family member satisfaction regarding critically ill patients in medical and surgical ICUs and their predicting factors.</p><p><strong>Results: </strong>This combined retrospective and prospective cohort study was conducted at a tertiary academic university-affiliated medical center. Patients admitted to the adult ICUs and had CEC between January 1, 2013, and December 31, 2020, were eligible. A total of 1,150 adult patients were included, with 822 in the medical and 328 in the surgical ICU. After the implementation of mandatory CEC policy, resource use in both ICUs deceased biannually. Medical ICU has significantly longer total length of stay (LOS), days of ventilator use, and days from ICU admission to ethics consultation than surgical ICU. Advanced cancer and the episode of cardiac arrest mainly predicted ICU LOS and resource use in the medical ICU, whereas the Glasgow Coma Scale (GCS) score was the main predicting factor for surgical ICU. Secular trends for incidence rates of ethical conflicts decreased biannually in both ICUs. In general, higher incidence rates of ethical conflicts were observed in the surgical ICU. The predicting factors for ethical conflicts in the medical ICU included age, patients with advanced cancer, patients who received inotropes or vasopressors, and the GCS score, whereas in the surgical ICU, the marital status and GCS score were the main predicting factors. Family members in both ICUs were highly satisfied with the CEC team.</p><p><strong>Conclusion: </strong>Medical and surgical ICUs exhibited different impacts on resource use and ethical conflicts after the implementation of mandatory CEC policy. Our results provide CEC and clinical teams with guidelines to approach the distinct issues within various specialties. The institution should consider implementing mandatory CEC policy and developing special educational and training programs for various specialties to provide the best quality of end-of-life care in the ICUs.</p><p><strong>Trial registration: </strong>The ClinicalTrials.gov Identifier is NCT04926610.</p>","PeriodicalId":55348,"journal":{"name":"BMC Medical Ethics","volume":"26 1","pages":"110"},"PeriodicalIF":3.1000,"publicationDate":"2025-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12318408/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Medical Ethics","FirstCategoryId":"98","ListUrlMain":"https://doi.org/10.1186/s12910-025-01268-4","RegionNum":1,"RegionCategory":"哲学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ETHICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Mandatory clinical ethics consultation (CEC) is initiated under specific circumstances when required by institutional policies. Medical and surgical intensive care units (ICUs) have various characteristics. Studies on whether mandatory CEC have different impacts on medical and surgical ICUs are limited. This study aimed to investigate the impacts of mandatory CEC on resource use and ethical conflicts as well as family member satisfaction regarding critically ill patients in medical and surgical ICUs and their predicting factors.
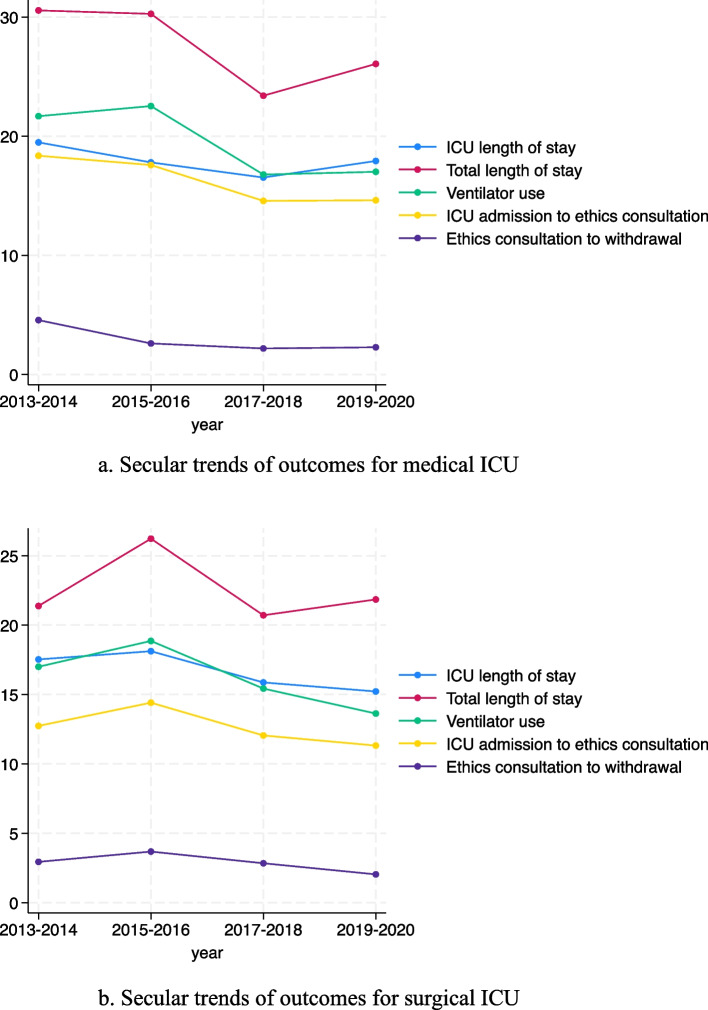
Results: This combined retrospective and prospective cohort study was conducted at a tertiary academic university-affiliated medical center. Patients admitted to the adult ICUs and had CEC between January 1, 2013, and December 31, 2020, were eligible. A total of 1,150 adult patients were included, with 822 in the medical and 328 in the surgical ICU. After the implementation of mandatory CEC policy, resource use in both ICUs deceased biannually. Medical ICU has significantly longer total length of stay (LOS), days of ventilator use, and days from ICU admission to ethics consultation than surgical ICU. Advanced cancer and the episode of cardiac arrest mainly predicted ICU LOS and resource use in the medical ICU, whereas the Glasgow Coma Scale (GCS) score was the main predicting factor for surgical ICU. Secular trends for incidence rates of ethical conflicts decreased biannually in both ICUs. In general, higher incidence rates of ethical conflicts were observed in the surgical ICU. The predicting factors for ethical conflicts in the medical ICU included age, patients with advanced cancer, patients who received inotropes or vasopressors, and the GCS score, whereas in the surgical ICU, the marital status and GCS score were the main predicting factors. Family members in both ICUs were highly satisfied with the CEC team.
Conclusion: Medical and surgical ICUs exhibited different impacts on resource use and ethical conflicts after the implementation of mandatory CEC policy. Our results provide CEC and clinical teams with guidelines to approach the distinct issues within various specialties. The institution should consider implementing mandatory CEC policy and developing special educational and training programs for various specialties to provide the best quality of end-of-life care in the ICUs.
Trial registration: The ClinicalTrials.gov Identifier is NCT04926610.
期刊介绍:
BMC Medical Ethics is an open access journal publishing original peer-reviewed research articles in relation to the ethical aspects of biomedical research and clinical practice, including professional choices and conduct, medical technologies, healthcare systems and health policies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


