{"title":"Rapid, season-specific PCR testing versus traditional diagnostics for pneumonia in the emergency department.","authors":"Yangxiu Yu, Qiuping Li","doi":"10.1186/s12890-025-03843-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Traditional culture-based diagnostics for emergency-department (ED) pneumonia are slow and season-agnostic, delaying targeted therapy. We evaluated whether season-tailored multiplex PCR panels accelerate pathogen identification and improve antibiotic stewardship.</p><p><strong>Methods: </strong>In a single-center, prospective study, adults with radiographically confirmed pneumonia were enrolled consecutively and allocated by a rotating week-on/week-off schedule to either a seasonal PCR panel or conventional diagnostics. Primary outcomes were (i) time to final pathogen report and (ii) diagnostic yield (≥ 1 pathogen detected). Secondary outcomes included empiric-antibiotic appropriateness within 24 h, regimen changes ≤ 72 h, antibiotic duration, length of stay (LOS) and 30-day mortality.</p><p><strong>Results: </strong>Among 282 analyzable patients (spring = 140; autumn-winter = 142), PCR slashed turnaround time from 48 h to 12 h in spring and from 50 h to 14 h in autumn-winter (median difference - 36 h, 95% CI: - 42 to - 30; p < 0.001). Diagnostic yield rose from 61.6 to 80.6% in spring and from 56.8 to 80.0% in winter (risk differences 19.0 pp and 22.3 pp, respectively; both p < 0.01). In the winter cohort, guideline-concordant empiric therapy increased (78.7% vs. 64.9%; +13.8 pp) and antibiotic changes ≤ 72 h fell (14.7% vs. 28.4%; - 13.7 pp). Mean antibiotic courses shortened by 1.5-1.7 days across seasons, while LOS showed a non-significant 1-2-day reduction. Thirty-day mortality did not differ. Effects were consistent in older adults (≥ 65 y) and patients with COPD.</p><p><strong>Conclusions: </strong>Locally adapted, season-specific multiplex PCR panels deliver near-four-fold faster, higher-yield pathogen detection and support measurable stewardship gains without compromising safety. Implementation in other settings should consider local pathogen seasonality, workflow, and cost structures.</p>","PeriodicalId":9148,"journal":{"name":"BMC Pulmonary Medicine","volume":"25 1","pages":"372"},"PeriodicalIF":2.8000,"publicationDate":"2025-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12318422/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Pulmonary Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12890-025-03843-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Traditional culture-based diagnostics for emergency-department (ED) pneumonia are slow and season-agnostic, delaying targeted therapy. We evaluated whether season-tailored multiplex PCR panels accelerate pathogen identification and improve antibiotic stewardship.
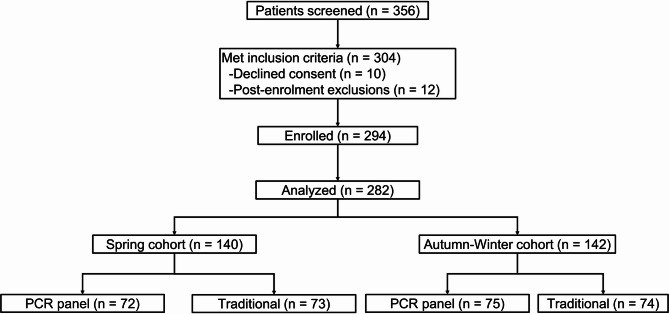
Methods: In a single-center, prospective study, adults with radiographically confirmed pneumonia were enrolled consecutively and allocated by a rotating week-on/week-off schedule to either a seasonal PCR panel or conventional diagnostics. Primary outcomes were (i) time to final pathogen report and (ii) diagnostic yield (≥ 1 pathogen detected). Secondary outcomes included empiric-antibiotic appropriateness within 24 h, regimen changes ≤ 72 h, antibiotic duration, length of stay (LOS) and 30-day mortality.
Results: Among 282 analyzable patients (spring = 140; autumn-winter = 142), PCR slashed turnaround time from 48 h to 12 h in spring and from 50 h to 14 h in autumn-winter (median difference - 36 h, 95% CI: - 42 to - 30; p < 0.001). Diagnostic yield rose from 61.6 to 80.6% in spring and from 56.8 to 80.0% in winter (risk differences 19.0 pp and 22.3 pp, respectively; both p < 0.01). In the winter cohort, guideline-concordant empiric therapy increased (78.7% vs. 64.9%; +13.8 pp) and antibiotic changes ≤ 72 h fell (14.7% vs. 28.4%; - 13.7 pp). Mean antibiotic courses shortened by 1.5-1.7 days across seasons, while LOS showed a non-significant 1-2-day reduction. Thirty-day mortality did not differ. Effects were consistent in older adults (≥ 65 y) and patients with COPD.
Conclusions: Locally adapted, season-specific multiplex PCR panels deliver near-four-fold faster, higher-yield pathogen detection and support measurable stewardship gains without compromising safety. Implementation in other settings should consider local pathogen seasonality, workflow, and cost structures.
期刊介绍:
BMC Pulmonary Medicine is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of pulmonary and associated disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


