Outcomes in Older Patients After Switching to a Newer Anticoagulant or Remaining on Warfarin
IF 22.3
1区 医学
Q1 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 0
Abstract
Background
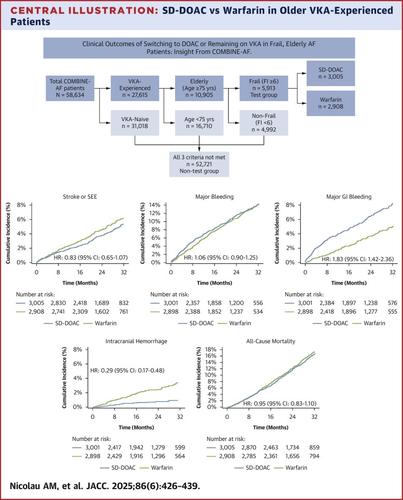
Whether frail, elderly patients with atrial fibrillation (AF) on a vitamin K antagonist (VKA) should switch to a direct-acting oral anticoagulant (DOAC) was studied in the FRAIL-AF trial and remains controversial.
Objectives
The purpose of this study was to evaluate, in the COMBINE-AF data set, the impact on clinical outcomes of switching frail, elderly AF patients from VKA to DOAC.
Methods
COMBINE-AF consists of individual patient-level data from 71,683 patients with AF in 4 randomized clinical trials comparing DOAC vs warfarin. Frailty was evaluated using a frailty index derived from a modified Rockwood’s Accumulation Model including 18 age-related conditions. Patients with a frailty index score above the median were considered frail. Prespecified outcomes were stroke or systemic embolic events, bleeding events, death, and a net clinical outcome combining these events.
Results
We identified 5,913 patients who were frail, elderly (age ≥75 years), and VKA-experienced and 52,721 patients who did not meet all 3 of these criteria. Patients were randomized to a standard-dose (SD) DOAC or warfarin. After 27 months median follow-up, there was no heterogeneity in treatment effect with SD-DOAC vs warfarin among those who met all 3 criteria vs those who did not for the endpoints of stroke or systemic embolic events (HR: 0.83 vs 0.81; Pint = 0.75) or for death (HR: 0.95 vs 0.91; Pint = 0.54). Major bleeding was similar with SD-DOAC vs warfarin in frail, elderly, VKA-experienced patients (HR: 1.06 [95% CI: 0.90-1.25]), while it was significantly reduced with SD-DOAC in patients without all 3 criteria (HR: 0.82 [95% CI: 0.76-0.89]; Pint = 0.007). Likewise, the net clinical outcome was similar in the frail, elderly, VKA-experienced patients with SD-DOAC vs warfarin (HR: 1.01 [95% CI: 0.91-1.13]), while significantly reduced with SD-DOAC patients without all 3 criteria (HR: 0.89 [95% CI: 0.85-0.93]; Pint = 0.028). Fatal and intracranial bleeding were significantly reduced with SD-DOAC in both subgroups to a similar degree (both Pint > 0.05), while gastrointestinal bleeding with SD-DOAC was increased to a greater degree in frail, elderly, VKA-experienced patients (HR: 1.83 [95% CI: 1.42-2.36]) compared with those without all 3 criteria (HR: 1.23 [95% CI: 1.09-1.39]; Pint = 0.006).
Conclusions
Frail, elderly, VKA-experienced patients with AF switched to SD-DOAC experienced significant reductions in stroke or systemic embolism, fatal and intracranial bleeding, and death. Gastrointestinal bleeding was increased with SD-DOAC, while major bleeding and the primary net clinical outcome were similar. Based on these findings, SD-DOAC is a reasonable choice for frail, elderly, VKA-experienced patients to reduce stroke and systemic embolism, death, and the most serious types of bleeding.
老年患者改用新型抗凝剂或继续使用华法林后的预后
背景:虚弱的老年心房颤动(AF)患者服用维生素K拮抗剂(VKA)是否应该切换到直接作用的口服抗凝剂(DOAC),在虚弱的心房颤动(AF)试验中进行了研究,但仍存在争议。目的:本研究的目的是在合并房颤的数据集中,评估虚弱的老年房颤患者从VKA转为DOAC对临床结果的影响。方法:combine -AF包括4项比较DOAC与华法林的随机临床试验中71683例房颤患者的个体患者水平数据。脆弱性评估使用脆弱性指数衍生自改良的Rockwood积累模型,包括18个与年龄相关的条件。虚弱指数评分高于中位数的患者被认为是虚弱的。预先指定的结局是中风或全身性栓塞事件、出血事件、死亡,以及结合这些事件的净临床结局。结果我们确定了5,913例体弱、老年(年龄≥75岁)和有vka经历的患者,以及52,721例不符合所有这3个标准的患者。患者被随机分配到标准剂量DOAC或华法林。中位随访27个月后,在卒中或系统性栓塞事件终点方面,符合所有3个标准的患者与不符合3个标准的患者相比,SD-DOAC与华法林的治疗效果没有异质性(HR: 0.83 vs 0.81;品脱= 0.75)或死亡(风险比:0.95 vs 0.91;品脱= 0.54)。SD-DOAC与华法林在体弱、老年、有vka经历的患者中大出血相似(HR: 1.06 [95% CI: 0.90-1.25]),而在没有所有3项标准的患者中,SD-DOAC显著减少大出血(HR: 0.82 [95% CI: 0.76-0.89];品脱= 0.007)。同样,SD-DOAC与华法林治疗的体弱、老年、有vka经历的患者的净临床结果相似(HR: 1.01 [95% CI: 0.91-1.13]),而没有所有3个标准的SD-DOAC患者的净临床结果显著降低(HR: 0.89 [95% CI: 0.85-0.93];品脱= 0.028)。SD-DOAC在两个亚组中均显著减少致死性出血和颅内出血,且减少程度相似(均为Pint >;0.05),而与没有所有3项标准的患者(HR: 1.23 [95% CI: 1.09-1.39])相比,虚弱、老年、有vka经历的患者(HR: 1.83 [95% CI: 1.42-2.36]) SD-DOAC的胃肠道出血增加程度更高;品脱= 0.006)。结论:体弱多病、老年、有vka经验的房颤患者改用SD-DOAC后,卒中或全身性栓塞、致命性和颅内出血以及死亡的发生率显著降低。SD-DOAC增加了胃肠道出血,而大出血和主要净临床结果相似。基于这些发现,SD-DOAC是体弱、老年、有vka经验的患者减少中风、全身性栓塞、死亡和最严重类型出血的合理选择。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

CiteScore
42.70
自引率
3.30%
发文量
5097
审稿时长
2-4 weeks
期刊介绍:
The Journal of the American College of Cardiology (JACC) publishes peer-reviewed articles highlighting all aspects of cardiovascular disease, including original clinical studies, experimental investigations with clear clinical relevance, state-of-the-art papers and viewpoints.
Content Profile:
-Original Investigations
-JACC State-of-the-Art Reviews
-JACC Review Topics of the Week
-Guidelines & Clinical Documents
-JACC Guideline Comparisons
-JACC Scientific Expert Panels
-Cardiovascular Medicine & Society
-Editorial Comments (accompanying every Original Investigation)
-Research Letters
-Fellows-in-Training/Early Career Professional Pages
-Editor’s Pages from the Editor-in-Chief or other invited thought leaders
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


