Sigbjorn Sabo, Håkon Pettersen, Gunn C Bøen, Even O Jakobsen, Per K Langøy, Hans O Nilsen, David Pasdeloup, Erik Smistad, Andreas Østvik, Lasse Løvstakken, Stian Stølen, Bjørnar Grenne, Håvard Dalen, Espen Holte
{"title":"Real-time guidance and automated measurements using deep learning to improve echocardiographic assessment of left ventricular size and function.","authors":"Sigbjorn Sabo, Håkon Pettersen, Gunn C Bøen, Even O Jakobsen, Per K Langøy, Hans O Nilsen, David Pasdeloup, Erik Smistad, Andreas Østvik, Lasse Løvstakken, Stian Stølen, Bjørnar Grenne, Håvard Dalen, Espen Holte","doi":"10.1093/ehjimp/qyaf094","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The low reproducibility of echocardiographic measurements challenges the identification of subtle changes in left ventricular (LV) function. Deep learning (DL) methods enable real-time analysis of acquisitions and may improve echocardiography. The aim of this study was to evaluate the impact of DL-based guidance and automated measurements on the reproducibility of LV global longitudinal strain (GLS), end-diastolic (EDV) and end-systolic (ESV) volume, and ejection fraction (EF).</p><p><strong>Methods and results: </strong>Forty-six patients (24 breast cancer and 22 general cardiology patients) were included and underwent four consecutive echocardiograms. Six were included twice, totalling 52 inclusions and 208 echocardiograms. One sonographer-cardiologist pair used DL guidance and measurements (DL group), while another did not use DL tools and performed manual measurements (manual group). DL group recordings were also measured using a commercially available DL-based EF tool. For GLS, the DL group had a 30% lower test-retest variability than the manual group (minimal detectable change 2.0 vs. 2.9, <i>P</i> = 0.036). LV volumes had ∼40% lower minimal detectable changes in the DL group vs. the manual group (32 mL vs. 52 mL for EDV and 18 mL vs. 32 mL for ESV, <i>P</i> ≤ 0.006). This did not translate to a significant improvement in EF reproducibility in the DL group. The benchmarking method showed similar results compared with the manual group.</p><p><strong>Conclusion: </strong>Combining real-time DL guidance with automated measurements improved the reproducibility of LV size and function measurements compared with usual care, but future studies are needed to evaluate its clinical effect.</p><p><strong>Trial registration number: </strong>NCT06310330.</p>","PeriodicalId":94317,"journal":{"name":"European heart journal. Imaging methods and practice","volume":"3 2","pages":"qyaf094"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12311362/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Imaging methods and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjimp/qyaf094","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
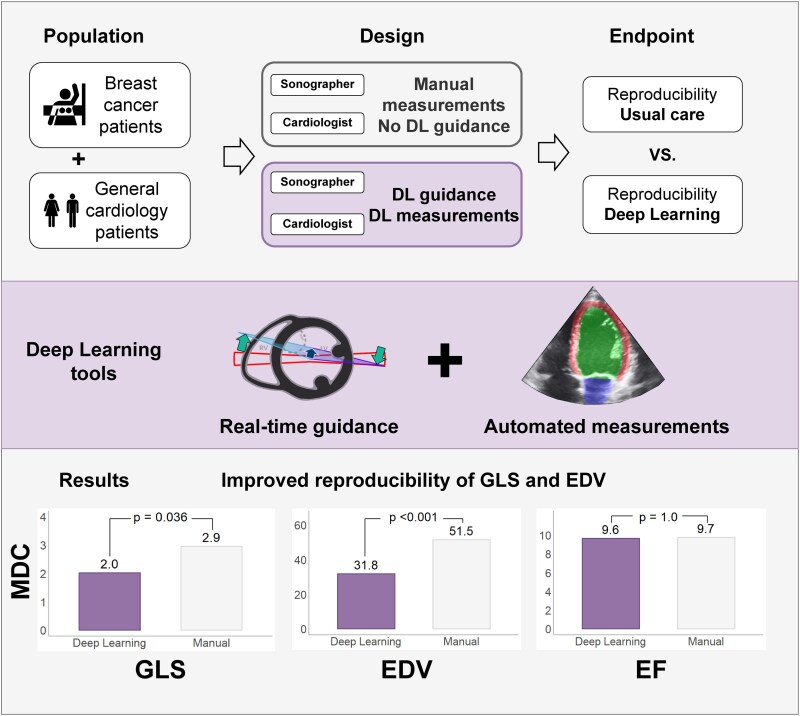
Aims: The low reproducibility of echocardiographic measurements challenges the identification of subtle changes in left ventricular (LV) function. Deep learning (DL) methods enable real-time analysis of acquisitions and may improve echocardiography. The aim of this study was to evaluate the impact of DL-based guidance and automated measurements on the reproducibility of LV global longitudinal strain (GLS), end-diastolic (EDV) and end-systolic (ESV) volume, and ejection fraction (EF).
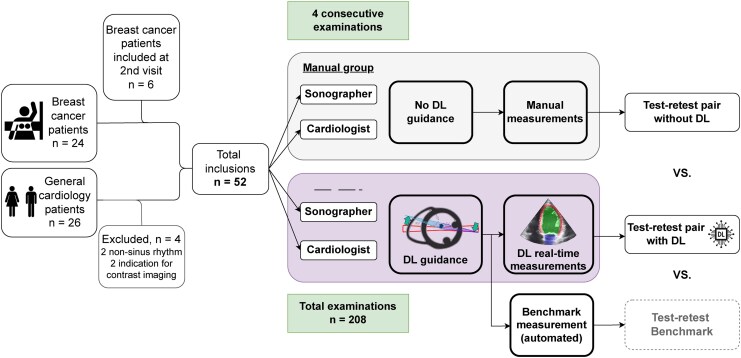
Methods and results: Forty-six patients (24 breast cancer and 22 general cardiology patients) were included and underwent four consecutive echocardiograms. Six were included twice, totalling 52 inclusions and 208 echocardiograms. One sonographer-cardiologist pair used DL guidance and measurements (DL group), while another did not use DL tools and performed manual measurements (manual group). DL group recordings were also measured using a commercially available DL-based EF tool. For GLS, the DL group had a 30% lower test-retest variability than the manual group (minimal detectable change 2.0 vs. 2.9, P = 0.036). LV volumes had ∼40% lower minimal detectable changes in the DL group vs. the manual group (32 mL vs. 52 mL for EDV and 18 mL vs. 32 mL for ESV, P ≤ 0.006). This did not translate to a significant improvement in EF reproducibility in the DL group. The benchmarking method showed similar results compared with the manual group.
Conclusion: Combining real-time DL guidance with automated measurements improved the reproducibility of LV size and function measurements compared with usual care, but future studies are needed to evaluate its clinical effect.
目的:超声心动图测量的低再现性对左心室(LV)功能细微变化的识别提出了挑战。深度学习(DL)方法能够实时分析采集,并可能改善超声心动图。本研究的目的是评估基于dl的引导和自动测量对左室整体纵向应变(GLS)、舒张末期(EDV)和收缩末期(ESV)体积和射血分数(EF)的再现性的影响。方法和结果:纳入46例患者(24例乳腺癌患者和22例普通心脏病患者),并连续进行4次超声心动图检查。6例纳入两次,共52例,超声心动图208例。一组超声医师-心脏科医师使用DL指导和测量(DL组),而另一组不使用DL工具并进行手动测量(手动组)。DL组记录也使用市售的基于DL的EF工具进行测量。对于GLS, DL组的重测变异性比手动组低30%(最小可检测变化2.0 vs 2.9, P = 0.036)。DL组的LV体积最小可检测变化比手动组低40% (EDV为32 mL vs 52 mL, ESV为18 mL vs 32 mL, P≤0.006)。这并没有转化为DL组EF重现性的显著改善。与手动组相比,基准测试方法显示了相似的结果。结论:与常规护理相比,实时DL引导与自动测量相结合提高了左室大小和功能测量的可重复性,但其临床效果有待进一步研究评价。试验注册号:NCT06310330。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


