Pankaj Garg, Aradhai Bana, Gareth Matthews, Tiya Bali, Rui Li, Zia Mehmood, Liang Zhong, Rob J van der Geest, Sven Plein, John P Greenwood, Peter Swoboda
{"title":"Haemodynamic implications of cardiovascular magnetic resonance pulmonary capillary wedge pressure in acute myocardial infarction.","authors":"Pankaj Garg, Aradhai Bana, Gareth Matthews, Tiya Bali, Rui Li, Zia Mehmood, Liang Zhong, Rob J van der Geest, Sven Plein, John P Greenwood, Peter Swoboda","doi":"10.1093/ehjimp/qyaf086","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Cardiovascular magnetic resonance (CMR)-derived pulmonary capillary wedge pressure (PCWP) has demonstrated diagnostic and prognostic utility in heart failure patients. However, its clinical value in acute myocardial infarction (AMI) remains undetermined. This study investigates the relationship between CMR-derived PCWP, myocardial injury, and left ventricular (LV) remodelling in re-perfused acute ST-elevation myocardial infarction (STEMI).</p><p><strong>Methods and results: </strong>Sixty-nine patients with STEMI underwent CMR within 48 h and at 3 months. PCWP was estimated using the sex-specific equation: CMR PCWP: 5.7591 + (0.07505 × left atrial volume) [0.05289 × left ventricular mass (LVM)] - (1.9927 × sex) [female = 0; male = 1], where LAV is left atrial volume (mL) and LVM is left ventricular mass (g). LV remodelling was assessed via changes in LV end-diastolic volume (LVEDV) and ejection fraction (LVEF). Patients with high CMR PCWP (≥18 mmHg) exhibited greater myocardial scar burden (28.5% vs. 17.2%, <i>P</i> = 0.0008) and microvascular obstruction (7.6% vs. 2.5%, <i>P</i> < 0.0001). They also had higher acute LVEDV (193.7 ± 39.7 vs. 158.0 ± 29.5 mL, <i>P</i> < 0.0001) and lower LVEF (41.4 ± 10.4% vs. 48.5 ± 9.2%, <i>P</i> = 0.0066). At follow-up, higher baseline CMR PCWP was associated with greater LV remodelling (<i>P</i> < 0.0001) and persistently reduced LVEF (45.4 ± 10.2% vs. 55.0 ± 10.3%, <i>P</i> = 0.0005). Regression analysis confirmed baseline PCWP as an independent predictor of follow-up LVEF (<i>P</i> = 0.0036).</p><p><strong>Conclusion: </strong>CMR-derived PCWP may be a valuable biomarker in STEMI, identifying patients at risk of adverse remodelling and LV dysfunction. Its integration into clinical practice may enhance risk stratification and guide targeted therapies.</p>","PeriodicalId":94317,"journal":{"name":"European heart journal. Imaging methods and practice","volume":"3 2","pages":"qyaf086"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12311366/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Imaging methods and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjimp/qyaf086","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Cardiovascular magnetic resonance (CMR)-derived pulmonary capillary wedge pressure (PCWP) has demonstrated diagnostic and prognostic utility in heart failure patients. However, its clinical value in acute myocardial infarction (AMI) remains undetermined. This study investigates the relationship between CMR-derived PCWP, myocardial injury, and left ventricular (LV) remodelling in re-perfused acute ST-elevation myocardial infarction (STEMI).
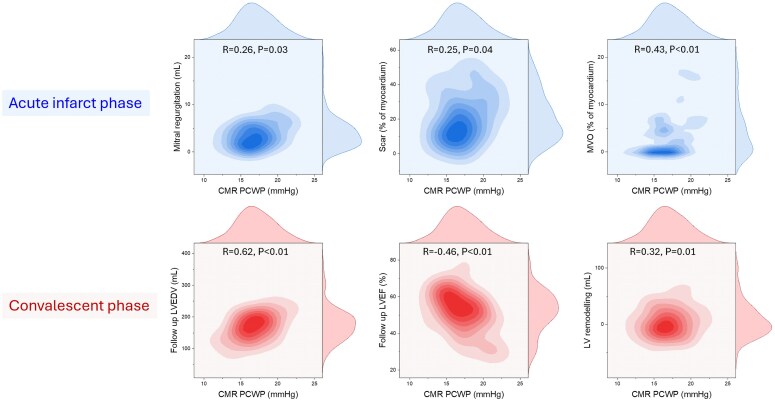
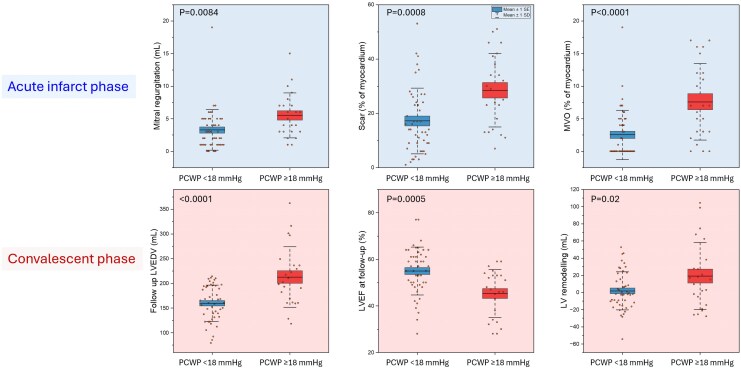
Methods and results: Sixty-nine patients with STEMI underwent CMR within 48 h and at 3 months. PCWP was estimated using the sex-specific equation: CMR PCWP: 5.7591 + (0.07505 × left atrial volume) [0.05289 × left ventricular mass (LVM)] - (1.9927 × sex) [female = 0; male = 1], where LAV is left atrial volume (mL) and LVM is left ventricular mass (g). LV remodelling was assessed via changes in LV end-diastolic volume (LVEDV) and ejection fraction (LVEF). Patients with high CMR PCWP (≥18 mmHg) exhibited greater myocardial scar burden (28.5% vs. 17.2%, P = 0.0008) and microvascular obstruction (7.6% vs. 2.5%, P < 0.0001). They also had higher acute LVEDV (193.7 ± 39.7 vs. 158.0 ± 29.5 mL, P < 0.0001) and lower LVEF (41.4 ± 10.4% vs. 48.5 ± 9.2%, P = 0.0066). At follow-up, higher baseline CMR PCWP was associated with greater LV remodelling (P < 0.0001) and persistently reduced LVEF (45.4 ± 10.2% vs. 55.0 ± 10.3%, P = 0.0005). Regression analysis confirmed baseline PCWP as an independent predictor of follow-up LVEF (P = 0.0036).
Conclusion: CMR-derived PCWP may be a valuable biomarker in STEMI, identifying patients at risk of adverse remodelling and LV dysfunction. Its integration into clinical practice may enhance risk stratification and guide targeted therapies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


