Nasser Malekpour Alamdari, Iman Ansari, Maede Karimian, Elnaz Babakhani, Sara Hatami, Parisa Mohammadsadeghi, Maryam Abbasi
{"title":"Peritoneal Hydatid Cyst Mimicking Peritoneal Seeding; A Case Report.","authors":"Nasser Malekpour Alamdari, Iman Ansari, Maede Karimian, Elnaz Babakhani, Sara Hatami, Parisa Mohammadsadeghi, Maryam Abbasi","doi":"10.30699/ijp.2025.2056341.3430","DOIUrl":null,"url":null,"abstract":"<p><strong>Background & objective: </strong>This study presents a rare case of hydatid cysts involving the liver, spleen, and peritoneum, in which clinical features and radiologic findings initially raised strong suspicion for abdominal malignancy with peritoneal seeding.</p><p><strong>Case presentation: </strong>A 64-year-old man presented with vague epigastric pain, weight loss, and iron deficiency anemia. Abdominal ultrasonography revealed multiple splenic lesions suggestive of hydatid cysts. Hydatid serology was negative. Chest CT was unremarkable. Abdominal and pelvic CT showed splenomegaly with cystic lesions, including a calcified cyst in segment VI of the liver. Numerous hypodense peritoneal nodules were identified, particularly in the mid-omentum and supraumbilical region. Differential diagnoses included hydatid disease, primary peritoneal neoplasms, and peritoneal metastases. Due to anemia, weight loss, and the suspicion of peritoneal carcinomatosis, hydatid disease alone could not fully account for the findings, prompting further diagnostic evaluation. Endoscopy and colonoscopy were unremarkable. The patient underwent exploratory laparotomy and splenectomy, along with partial omentectomy where hydatid involvement was suspected. Postoperatively, he was treated with albendazole 800 mg daily and discharged on postoperative day three. At 3- and 6-month follow-ups, the patient reported resolution of abdominal pain, and physical examinations were normal.</p><p><strong>Conclusion: </strong>Peritoneal hydatid disease is rare and can mimic peritoneal carcinomatosis, leading to diagnostic uncertainty and treatment delay. Surgical excision followed by antiparasitic therapy remains the cornerstone of management.</p>","PeriodicalId":38900,"journal":{"name":"Iranian Journal of Pathology","volume":"20 3","pages":"330-334"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12308191/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Iranian Journal of Pathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.30699/ijp.2025.2056341.3430","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background & objective: This study presents a rare case of hydatid cysts involving the liver, spleen, and peritoneum, in which clinical features and radiologic findings initially raised strong suspicion for abdominal malignancy with peritoneal seeding.
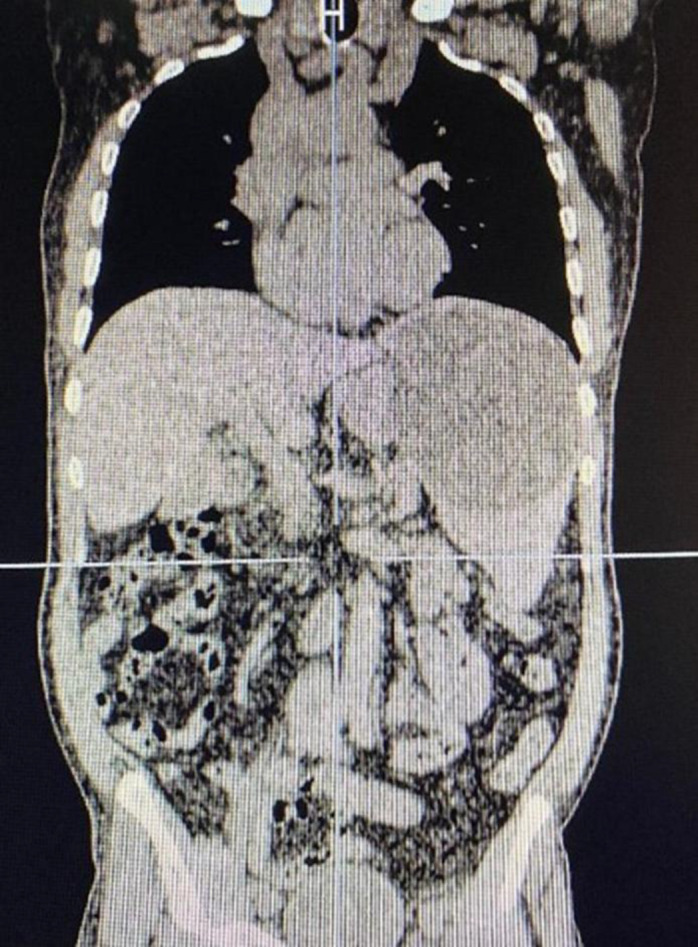
Case presentation: A 64-year-old man presented with vague epigastric pain, weight loss, and iron deficiency anemia. Abdominal ultrasonography revealed multiple splenic lesions suggestive of hydatid cysts. Hydatid serology was negative. Chest CT was unremarkable. Abdominal and pelvic CT showed splenomegaly with cystic lesions, including a calcified cyst in segment VI of the liver. Numerous hypodense peritoneal nodules were identified, particularly in the mid-omentum and supraumbilical region. Differential diagnoses included hydatid disease, primary peritoneal neoplasms, and peritoneal metastases. Due to anemia, weight loss, and the suspicion of peritoneal carcinomatosis, hydatid disease alone could not fully account for the findings, prompting further diagnostic evaluation. Endoscopy and colonoscopy were unremarkable. The patient underwent exploratory laparotomy and splenectomy, along with partial omentectomy where hydatid involvement was suspected. Postoperatively, he was treated with albendazole 800 mg daily and discharged on postoperative day three. At 3- and 6-month follow-ups, the patient reported resolution of abdominal pain, and physical examinations were normal.
Conclusion: Peritoneal hydatid disease is rare and can mimic peritoneal carcinomatosis, leading to diagnostic uncertainty and treatment delay. Surgical excision followed by antiparasitic therapy remains the cornerstone of management.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


