A randomized controlled trial comparing treatment efficacy between rapid maxillary expansion and adenotonsillectomy in pediatric obstructive sleep apnea.
{"title":"A randomized controlled trial comparing treatment efficacy between rapid maxillary expansion and adenotonsillectomy in pediatric obstructive sleep apnea.","authors":"Chalermthai Aksilp, Pattaralapa Pechpongsai, Pavinee Intakorn, Chaiyapol Chaweewannakorn, Supatchai Boonpratham, Yodhathai Satravaha, Niwat Anuwongnukroh, Supakit Peanchitlertkajorn","doi":"10.1007/s11325-025-03427-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Adenotonsillectomy (AT) is usually recommended as the first-line therapy for pediatric obstructive sleep apnea (POSA). While AT treats soft tissue obstruction, it does not address the underlying skeletal abnormalities, such as maxillary constriction. Despite growing evidence supporting RME as a treatment option for POSA, a significant research gap remains. Therefore, we conducted a randomized controlled trial to compare treatment efficacy between RME and AT.</p><p><strong>Methods: </strong>This study recruited 24 children diagnosed with POSA and presented with concurrent significant adenotonsillar hypertrophy and transverse maxillary deficiency. Participants were randomly assigned to either AT or RME for treatment. All participants underwent Type I PSG at baseline and 6 months post-treatment. Additional assessments included dental and cephalometric analyses, the pediatric sleep questionnaire (PSQ), and the OSA-18 questionnaire. Baseline and endpoint comparisons between the two treatment groups were performed.</p><p><strong>Results: </strong>The median baseline AHI for the AT and RME groups was 7.0 (5.25-9.9) and 6.85 (5.6-8.05) events/hour, respectively. There was no significant difference between treatment groups in all parameters at baseline. The comparisons between pre- and post-treatment results showed significant improvements across multiple parameters, including AHI for both AT and RME. There was no significant difference in PSG parameters (AHI, LSAT, MSAT, and REM sleep time) and cure rate between RME and AT. The post-treatment AHI for the AT and RME groups was 1.4 (0.7-1.85) and 2.3 (1.15-5.7) events/hour, respectively. However, PSQ and OSA-18 scores were significantly higher for the RME group.</p><p><strong>Conclusion: </strong>RME and AT significantly improved sleep-related respiratory parameters in patients with POSA. RME demonstrated comparable efficacy to AT in reducing AHI and improving LAST, MSAT, and REM sleep time. However, AT provided significantly better improvement in clinical symptoms and quality of life.</p><p><strong>Trial registration: </strong>The registration of this randomized controlled trial was approved on August 24th, 2023, under the registration number TCTR20230824001.</p>","PeriodicalId":520777,"journal":{"name":"Sleep & breathing = Schlaf & Atmung","volume":"29 4","pages":"256"},"PeriodicalIF":2.0000,"publicationDate":"2025-07-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12310760/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Sleep & breathing = Schlaf & Atmung","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s11325-025-03427-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Adenotonsillectomy (AT) is usually recommended as the first-line therapy for pediatric obstructive sleep apnea (POSA). While AT treats soft tissue obstruction, it does not address the underlying skeletal abnormalities, such as maxillary constriction. Despite growing evidence supporting RME as a treatment option for POSA, a significant research gap remains. Therefore, we conducted a randomized controlled trial to compare treatment efficacy between RME and AT.
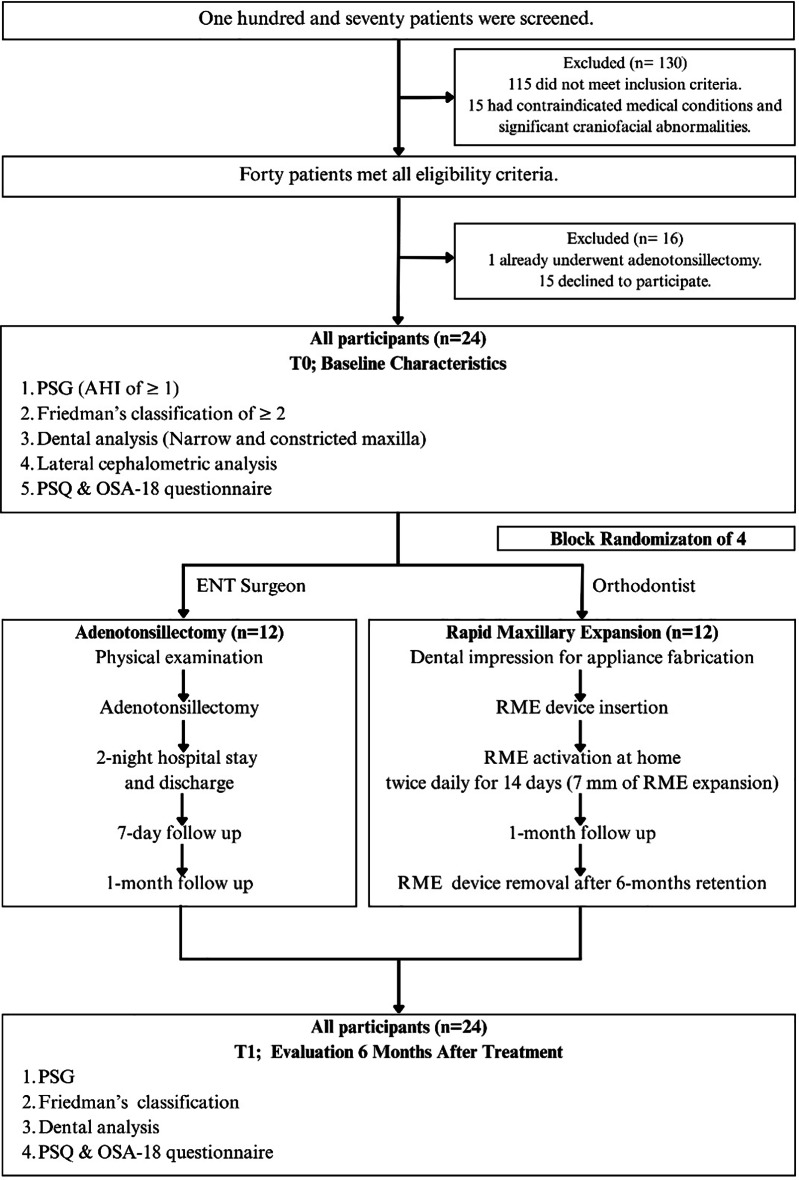
Methods: This study recruited 24 children diagnosed with POSA and presented with concurrent significant adenotonsillar hypertrophy and transverse maxillary deficiency. Participants were randomly assigned to either AT or RME for treatment. All participants underwent Type I PSG at baseline and 6 months post-treatment. Additional assessments included dental and cephalometric analyses, the pediatric sleep questionnaire (PSQ), and the OSA-18 questionnaire. Baseline and endpoint comparisons between the two treatment groups were performed.
Results: The median baseline AHI for the AT and RME groups was 7.0 (5.25-9.9) and 6.85 (5.6-8.05) events/hour, respectively. There was no significant difference between treatment groups in all parameters at baseline. The comparisons between pre- and post-treatment results showed significant improvements across multiple parameters, including AHI for both AT and RME. There was no significant difference in PSG parameters (AHI, LSAT, MSAT, and REM sleep time) and cure rate between RME and AT. The post-treatment AHI for the AT and RME groups was 1.4 (0.7-1.85) and 2.3 (1.15-5.7) events/hour, respectively. However, PSQ and OSA-18 scores were significantly higher for the RME group.
Conclusion: RME and AT significantly improved sleep-related respiratory parameters in patients with POSA. RME demonstrated comparable efficacy to AT in reducing AHI and improving LAST, MSAT, and REM sleep time. However, AT provided significantly better improvement in clinical symptoms and quality of life.
Trial registration: The registration of this randomized controlled trial was approved on August 24th, 2023, under the registration number TCTR20230824001.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


