Intertruncal versus classical approach to supraclavicular brachial plexus block on sensory-motor blockade for upper extremity surgery: a randomized controlled non-inferiority trial.
{"title":"Intertruncal versus classical approach to supraclavicular brachial plexus block on sensory-motor blockade for upper extremity surgery: a randomized controlled non-inferiority trial.","authors":"Zhipeng Wang, Jinyan Guo, Hanbin Xie, Guoliang Sun, Jianqiang Guan, Weifeng Yao, Quehua Luo","doi":"10.4097/kja.24526","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>As the characteristics of the intertruncal approach to the supraclavicular block (IA-SCB) are uncertain, we aimed to compare its effect on sensory-motor blockade with that of the classical approach (CA) within 30 min post-block.</p><p><strong>Methods: </strong>In total, 122 patients undergoing elbow, forearm, wrist, or hand surgery were randomly assigned to receive CA-SCB or IA-SCB. Both groups received identical local anesthetic agents (1% lidocaine and 0.5% ropivacaine) in 25 ml total. The IA-SCB group received 15 ml between the middle and inferior trunks and 10 ml between the superior and middle trunks, while the CA-SCB group received 15 ml in the corner pocket and 10 ml in the center of the neural clusters. Sensory-motor blockade of all four terminal nerves was assessed every 5 min for 30 min. The non-inferiority threshold aimed to exclude the possibility that the IA-SCB was > 5% inferior to the CA-SCB in terms of the proportion of patients with complete sensory blockade at 20 min post-block.</p><p><strong>Results: </strong>Complete sensory blockade at 20 min post-block was 79.3% and 72.7% with the CA-SCB and IA-SCB, respectively, exceeding the non-inferiority margin of -5% (-6.6%, 95% CI [-22.3% to 9.1%]; P value for non-inferiority = 0.206). Additionally, the IA-SCB showed an inferior musculocutaneous nerve blockade, longer performance time, and higher incidence of hemidiaphragmatic paresis.</p><p><strong>Conclusions: </strong>Our findings do not confirm the non-inferiority of the IA-SCB to the CA-SCB in achieving complete sensory blockade at 20 min post-block. Further research may be necessary to establish its efficacy in regional anesthesia.</p>","PeriodicalId":17855,"journal":{"name":"Korean Journal of Anesthesiology","volume":"78 4","pages":"321-330"},"PeriodicalIF":6.3000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12326560/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Anesthesiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4097/kja.24526","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/19 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: As the characteristics of the intertruncal approach to the supraclavicular block (IA-SCB) are uncertain, we aimed to compare its effect on sensory-motor blockade with that of the classical approach (CA) within 30 min post-block.
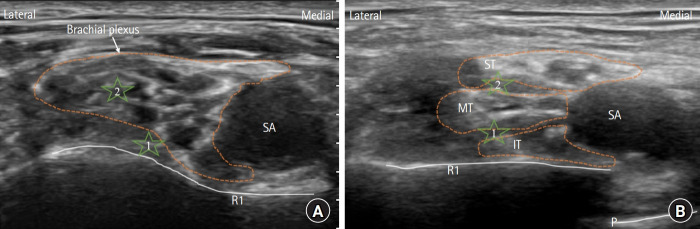
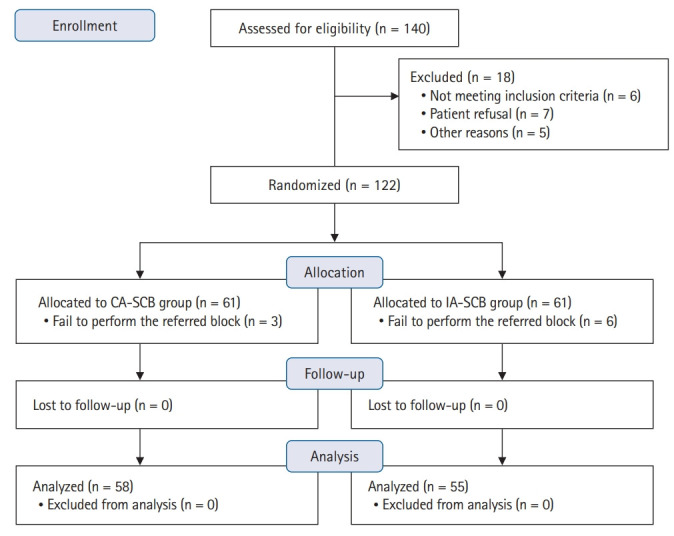
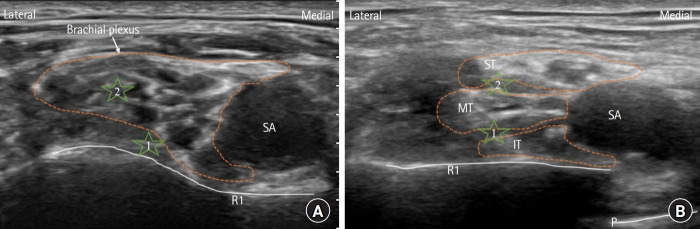
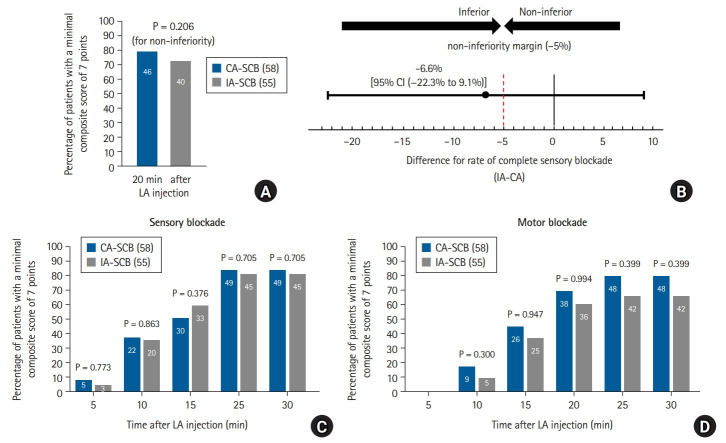
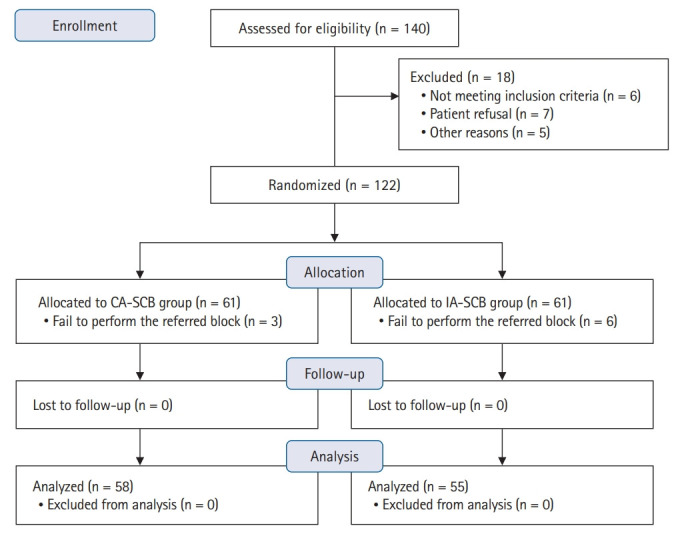
Methods: In total, 122 patients undergoing elbow, forearm, wrist, or hand surgery were randomly assigned to receive CA-SCB or IA-SCB. Both groups received identical local anesthetic agents (1% lidocaine and 0.5% ropivacaine) in 25 ml total. The IA-SCB group received 15 ml between the middle and inferior trunks and 10 ml between the superior and middle trunks, while the CA-SCB group received 15 ml in the corner pocket and 10 ml in the center of the neural clusters. Sensory-motor blockade of all four terminal nerves was assessed every 5 min for 30 min. The non-inferiority threshold aimed to exclude the possibility that the IA-SCB was > 5% inferior to the CA-SCB in terms of the proportion of patients with complete sensory blockade at 20 min post-block.
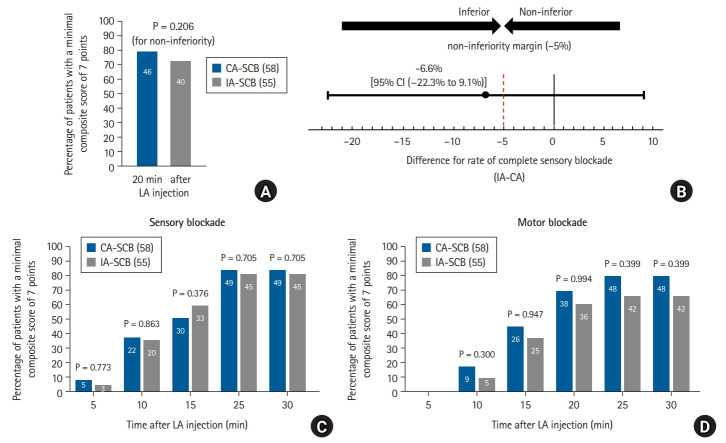
Results: Complete sensory blockade at 20 min post-block was 79.3% and 72.7% with the CA-SCB and IA-SCB, respectively, exceeding the non-inferiority margin of -5% (-6.6%, 95% CI [-22.3% to 9.1%]; P value for non-inferiority = 0.206). Additionally, the IA-SCB showed an inferior musculocutaneous nerve blockade, longer performance time, and higher incidence of hemidiaphragmatic paresis.
Conclusions: Our findings do not confirm the non-inferiority of the IA-SCB to the CA-SCB in achieving complete sensory blockade at 20 min post-block. Further research may be necessary to establish its efficacy in regional anesthesia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


