{"title":"Streptococcal Pharyngitis Complicated by Clinically Significant Rheumatic Myopericarditis: A Case Report.","authors":"Amanda Nguyen, Garrett Cohen, Matthew Lam","doi":"10.1177/23247096251362985","DOIUrl":null,"url":null,"abstract":"<p><p>Acute rheumatic fever (ARF) is a complication of streptococcal pharyngitis that can present with cardiac, joint, skin, and neurological symptoms. Cardiac manifestations most often involve valvular dysfunction, but can also include myocarditis or pericarditis. Although advances in healthcare have reduced the prevalence of streptococcal pharyngitis, and subsequently ARF, individual cases and outbreaks can still occur. We present a case of rheumatic myopericarditis in a 60-year-old White male who initially presented to the emergency department with sore throat for 6 days. Initial workup was largely unremarkable, and no microbiological testing was performed at that time. He was diagnosed with presumed viral pharyngitis and discharged home with supportive care. He returned 1 week later with pleuritic mid-sternal chest pain and dyspnea. Laboratory tests were significant for elevated inflammatory markers, cardiac enzyme markers, anti-streptolysin O titers, and <i>Streptococcus pyogenes</i> bacteremia. Further evaluation revealed pericarditis, moderate pericardial effusion without tamponade, and reduced systolic function without valvular disease. The patient was diagnosed with rheumatic myopericarditis. Management included pericardial drainage, guideline-directed medical therapy for systolic heart failure and pericarditis, and primary treatment and secondary prevention of ARF with antibiotics. Currently, the patient's cardiac function has recovered, and he regularly follows up with his medical care team. Although less common in present times, clinicians are encouraged to consider streptococcal pharyngitis and ARF on the differential diagnosis for patients presenting with pharyngeal symptoms and subsequent cardiac manifestations, with or without valvular dysfunction. Primary and secondary prevention of ARF is paramount to maintaining the low incidence of this disease.</p>","PeriodicalId":16198,"journal":{"name":"Journal of investigative medicine high impact case reports","volume":"13 ","pages":"23247096251362985"},"PeriodicalIF":0.8000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317263/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of investigative medicine high impact case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23247096251362985","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/31 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
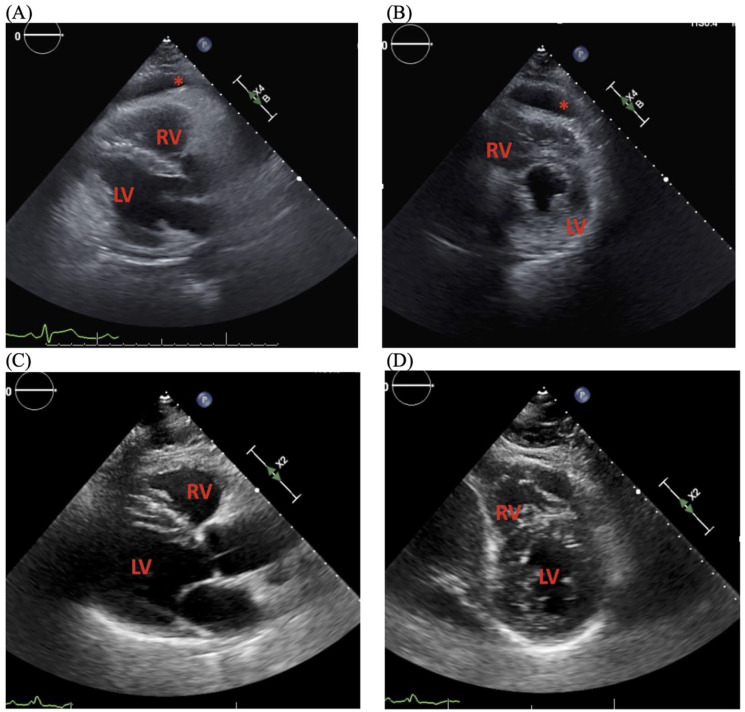
Acute rheumatic fever (ARF) is a complication of streptococcal pharyngitis that can present with cardiac, joint, skin, and neurological symptoms. Cardiac manifestations most often involve valvular dysfunction, but can also include myocarditis or pericarditis. Although advances in healthcare have reduced the prevalence of streptococcal pharyngitis, and subsequently ARF, individual cases and outbreaks can still occur. We present a case of rheumatic myopericarditis in a 60-year-old White male who initially presented to the emergency department with sore throat for 6 days. Initial workup was largely unremarkable, and no microbiological testing was performed at that time. He was diagnosed with presumed viral pharyngitis and discharged home with supportive care. He returned 1 week later with pleuritic mid-sternal chest pain and dyspnea. Laboratory tests were significant for elevated inflammatory markers, cardiac enzyme markers, anti-streptolysin O titers, and Streptococcus pyogenes bacteremia. Further evaluation revealed pericarditis, moderate pericardial effusion without tamponade, and reduced systolic function without valvular disease. The patient was diagnosed with rheumatic myopericarditis. Management included pericardial drainage, guideline-directed medical therapy for systolic heart failure and pericarditis, and primary treatment and secondary prevention of ARF with antibiotics. Currently, the patient's cardiac function has recovered, and he regularly follows up with his medical care team. Although less common in present times, clinicians are encouraged to consider streptococcal pharyngitis and ARF on the differential diagnosis for patients presenting with pharyngeal symptoms and subsequent cardiac manifestations, with or without valvular dysfunction. Primary and secondary prevention of ARF is paramount to maintaining the low incidence of this disease.
期刊介绍:
The AFMR is committed to enhancing the training and career development of our members and to furthering its mission to facilitate the conduct of research to improve medical care. Case reports represent an important avenue for trainees (interns, residents, and fellows) and early-stage faculty to demonstrate productive, scholarly activity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


