{"title":"Clinical and physiological characteristics of tremor in a large cohort of focal and segmental dystonia.","authors":"Zakia Jabarkheel, Aparna Wagle Shukla","doi":"10.3389/dyst.2024.12551","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Tremor is a frequent co-occurring feature in patients with dystonia, especially in focal and segmental dystonia. Clinical studies have shown that tremor is more commonly observed when dystonia spreads to contiguous body regions. However, there is insufficient characterization of tremor physiology in focal and segmental forms of dystonia. We aimed to ascertain the characteristics of tremor presenting in these specific subtypes.</p><p><strong>Methods: </strong>We enrolled dystonia patients with head and arm tremors presenting to our center. We categorized these participants as focal and segmental dystonia following the Movement Disorders Society guidelines. We recorded the frequency, amplitude, rhythmicity, burst duration, and discharge pattern on accelerometer and electromyography recordings. We compared the physiology of tremors in focal vs. segmental dystonia. We determined whether the physiology was affected by clinical features such as demographics, age at onset, dystonia duration, alcohol responsiveness, family history, and botulinum toxin responsiveness.</p><p><strong>Results: </strong>72 patients, mainly focal cervical dystonia and focal cervical + arm or cranial dystonia (segmental) were enrolled. In the analysis of the head tremor recordings (n = 66; frequency range 3-6.5 Hz), we found that focal vs. segmental dystonia comparisons revealed a significantly lower frequency (mean ± standard deviation; 4.0 ± 0.9 Hz vs. 4.7 ± 1.0 Hz; <i>p</i> = 0.02), lower amplitude (0.004 ± 0.008 g<sup>2</sup>/Hz vs. 0.006 ± 0.008 g<sup>2</sup>/Hz; <i>p</i> = 0.03) and longer muscle burst durations (111.1 ± 40.4 ms vs. 91.5 ± 24 ms; <i>p</i> = 0.04). In the analysis of arm tremor recordings (n = 31; frequency range 3.5-7 Hz), we found focal vs. segmental dystonia comparison revealed a lower amplitude (0.04 ± 0.07 g<sup>2</sup>/Hz vs. 0.06 ± 0.06 g<sup>2</sup>/Hz; <i>p</i> = 0.045). In the stepwise regression analysis, the age at evaluation (β - 0.44; <i>p</i> = 0.006) and age at onset (β - 0.61; <i>p</i> = 0.005) significantly predicted the head tremor frequency whereas the alcohol responsiveness tended to predict the amplitude of the head tremor (β - 0.5; <i>p</i> = 0.04) and the arm tremor (β - 0.6; <i>p</i> = 0.02).</p><p><strong>Conclusion: </strong>Our study found that the physiological characteristics of tremor in focal and segmental dystonia are somewhat distinct, suggesting that the spread of dystonia symptoms from one body region to another may have a bearing on the physiology of co-occurring tremor. The frequency of head tremors in younger participants was observed to be higher compared to older participants. The head and arm tremor tended be less severe in patients reporting alcohol responsiveness.</p>","PeriodicalId":72853,"journal":{"name":"Dystonia","volume":"3 ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12306709/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Dystonia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/dyst.2024.12551","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/9 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Tremor is a frequent co-occurring feature in patients with dystonia, especially in focal and segmental dystonia. Clinical studies have shown that tremor is more commonly observed when dystonia spreads to contiguous body regions. However, there is insufficient characterization of tremor physiology in focal and segmental forms of dystonia. We aimed to ascertain the characteristics of tremor presenting in these specific subtypes.
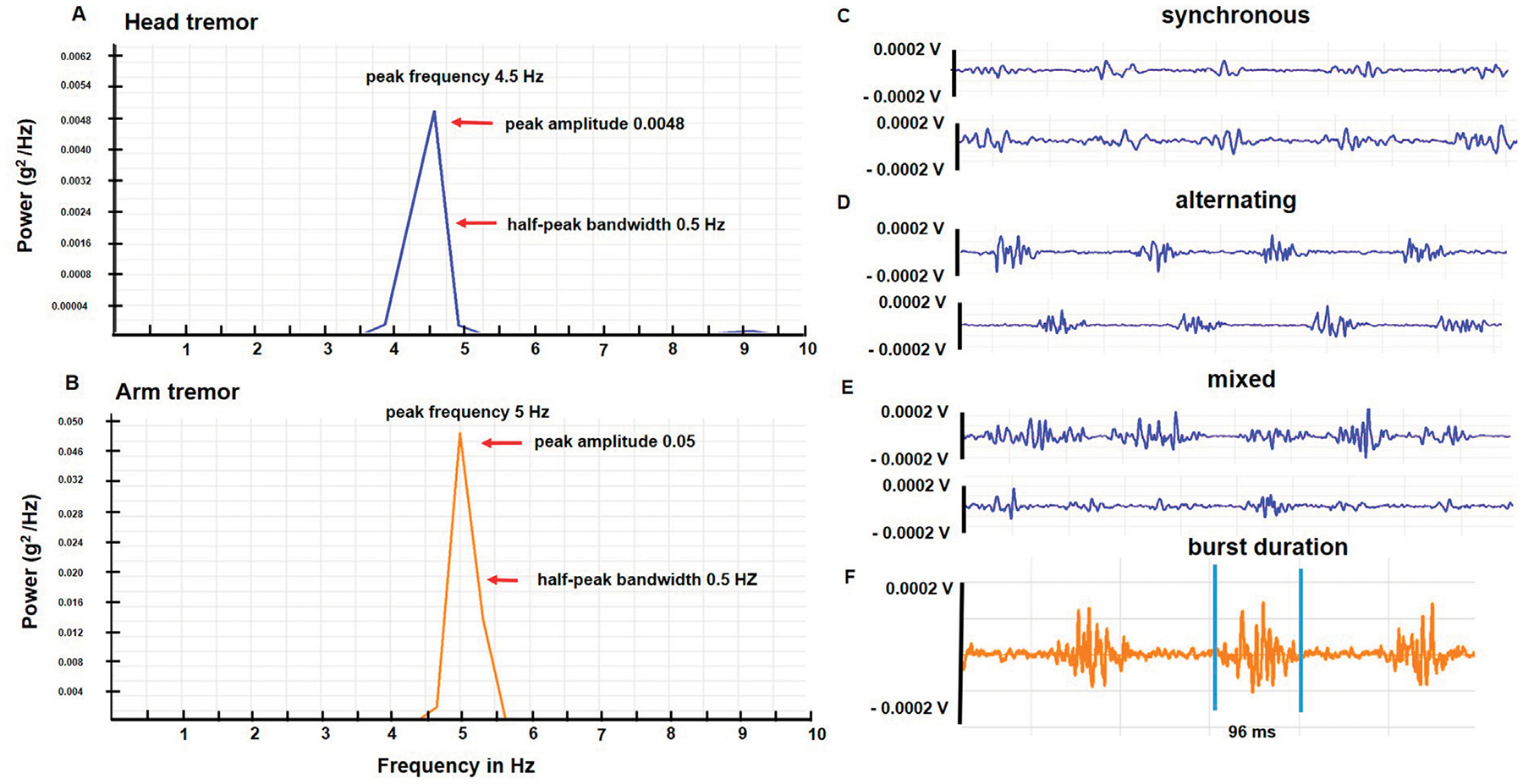
Methods: We enrolled dystonia patients with head and arm tremors presenting to our center. We categorized these participants as focal and segmental dystonia following the Movement Disorders Society guidelines. We recorded the frequency, amplitude, rhythmicity, burst duration, and discharge pattern on accelerometer and electromyography recordings. We compared the physiology of tremors in focal vs. segmental dystonia. We determined whether the physiology was affected by clinical features such as demographics, age at onset, dystonia duration, alcohol responsiveness, family history, and botulinum toxin responsiveness.
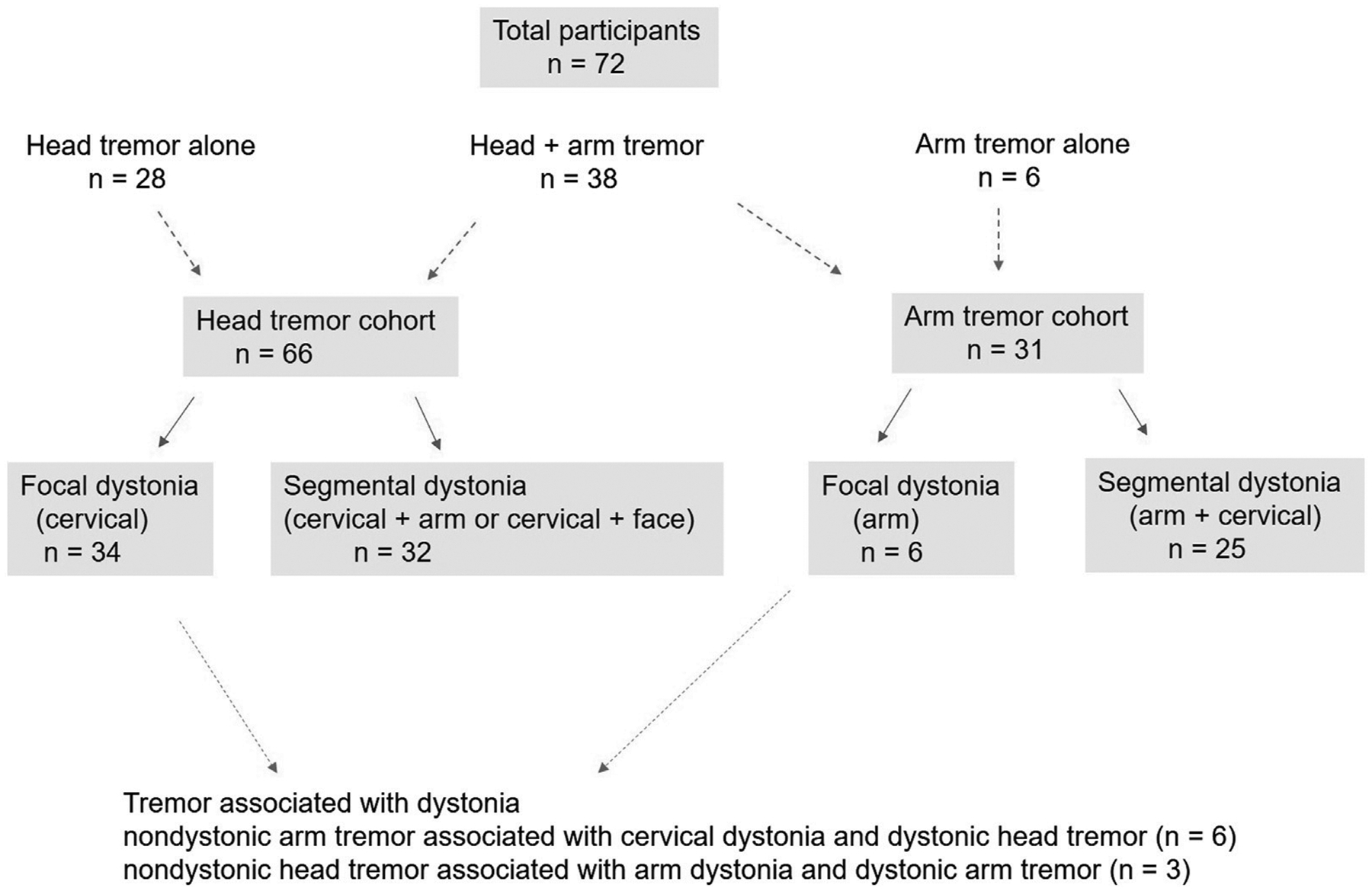
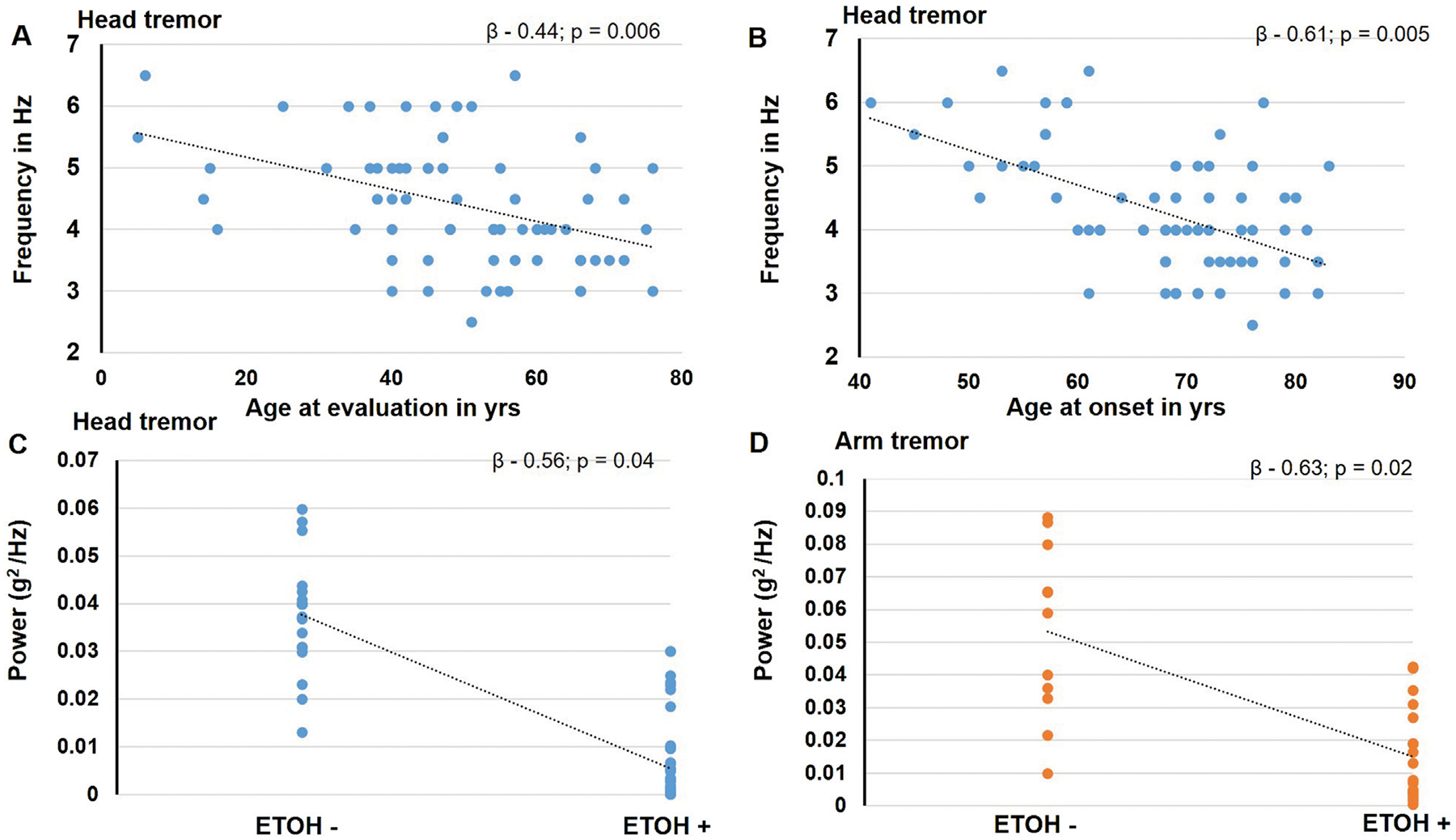
Results: 72 patients, mainly focal cervical dystonia and focal cervical + arm or cranial dystonia (segmental) were enrolled. In the analysis of the head tremor recordings (n = 66; frequency range 3-6.5 Hz), we found that focal vs. segmental dystonia comparisons revealed a significantly lower frequency (mean ± standard deviation; 4.0 ± 0.9 Hz vs. 4.7 ± 1.0 Hz; p = 0.02), lower amplitude (0.004 ± 0.008 g2/Hz vs. 0.006 ± 0.008 g2/Hz; p = 0.03) and longer muscle burst durations (111.1 ± 40.4 ms vs. 91.5 ± 24 ms; p = 0.04). In the analysis of arm tremor recordings (n = 31; frequency range 3.5-7 Hz), we found focal vs. segmental dystonia comparison revealed a lower amplitude (0.04 ± 0.07 g2/Hz vs. 0.06 ± 0.06 g2/Hz; p = 0.045). In the stepwise regression analysis, the age at evaluation (β - 0.44; p = 0.006) and age at onset (β - 0.61; p = 0.005) significantly predicted the head tremor frequency whereas the alcohol responsiveness tended to predict the amplitude of the head tremor (β - 0.5; p = 0.04) and the arm tremor (β - 0.6; p = 0.02).
Conclusion: Our study found that the physiological characteristics of tremor in focal and segmental dystonia are somewhat distinct, suggesting that the spread of dystonia symptoms from one body region to another may have a bearing on the physiology of co-occurring tremor. The frequency of head tremors in younger participants was observed to be higher compared to older participants. The head and arm tremor tended be less severe in patients reporting alcohol responsiveness.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


