Qianyu Shi, Jiazhi Zhu, Haijie Liang, Ruifeng Wang, Siyi Huang, Wei Guo, Tao Ji, Xiaodong Tang
{"title":"How precise is excision and reconstruction using 3D printing technology for total sacrectomy: accuracy validation in 9 consecutive cases.","authors":"Qianyu Shi, Jiazhi Zhu, Haijie Liang, Ruifeng Wang, Siyi Huang, Wei Guo, Tao Ji, Xiaodong Tang","doi":"10.1186/s41205-025-00295-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>With 3D printing technology, we can now use preoperative imaging for precise surgical plan. We can also use patient-specific surgical jig to improve the accuracy of osteotomy and 3D-printed custom-made endoprostheses combined with a screw-rod system to restore lumbosacral stability. The aim of this study was to evaluate the accuracy of 3D printing technology for precise osteotomy during total sacrectomy.</p><p><strong>Methods: </strong>Nine patients with primary malignant tumors of the sacrum who underwent total sacrectomy at our center were enrolled. Osteotomy was planned based on preoperative imaging (CT, MRI). Generally, an additional 8-10 mm margin beyond the tumor was determined by the fusion of MR and CT images. Patient-specific surgical jigs and 3D-printed sacral endoprostheses were then designed based on the planned osteotomy planes. Pre- and postoperative 3D models of the lumbosacral and pelvic regions were constructed using the fiducial registration model of 3D slicer software 5.1.0. Postoperative CT scans were compared with the planned osteomy planes based on preoperative CT scans, in order to evaluate the accuracy of the osteotomy and endoprosthetic reconstruction. For each patient, four levels of osteotomy planes were chosen, including the upper edge of the sacroiliac (SI) joint, the S1 and S2 foramen levels, and the caudal edge of the SI joint, for analyzing position and angular deviations between the preoperative plan and actual osteotomy along with the endoprosthesis position.</p><p><strong>Results: </strong>Pathological diagnoses included four cases of osteosarcoma, four cases of chordoma, and one case of Ewing sarcoma. All osteotomies in nine patients achieved R0 resection, as verified pathologically. An average angular deviation of 4.27° (interquartile range[IQR] 4.15) and an osteotomy position deviation of 4.00 mm (IQR 2.90) were observed. The mean angular deviations of the four levels were 3.50° (IQR 6.02), 3.86° (IQR 2.55), 4.81° (IQR 4.37), and 4.92° (IQR 3.27). The mean position deviations at the four levels were 3.15 mm (IQR 3.54), 3.55 mm (IQR 1.37), 4.26 mm (IQR 2.61), and 4.86 mm (IQR 3.93). No significant difference was found among the angular and position deviations at different levels. However, the proportions of individuals with position deviations > 2 mm and > 5 mm were significantly greater at the caudal end of the SI joint than at the upper end. All position deviations were within 8 mm. The average follow-up duration was 24.4 months. At the last follow-up, three patients experienced local recurrence, and one patient died of disease. All endoprostheses were in place without significant displacement. The mean Musculoskeletal Tumor Society scoring system (MSTS93) and MUD scores (function and sensation of lower limbs (M), urination and uriesthesia (U), and defecation and rectal sensation (D)) were 19.4 (16 to 24) and 16.3 (12 to 24), respectively.</p><p><strong>Conclusion: </strong>Notably, 3D-printed patient-specific surgical jigs exhibit high accuracy of osteotomy and lead to optimal surgical margin and reconstruction in total sacrectomy. Effective and reliable reconstruction can be achieved with a custom-made 3D-printed endoprosthesis. The application of 3D printing technology using patient-specific surgical jigs and the custom-made 3D-printed implants exhibited high surgical accuracy in total sacrectomy, as evidenced by accuracy validation.</p>","PeriodicalId":72036,"journal":{"name":"3D printing in medicine","volume":"11 1","pages":"42"},"PeriodicalIF":3.1000,"publicationDate":"2025-07-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12308921/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"3D printing in medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41205-025-00295-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Background: With 3D printing technology, we can now use preoperative imaging for precise surgical plan. We can also use patient-specific surgical jig to improve the accuracy of osteotomy and 3D-printed custom-made endoprostheses combined with a screw-rod system to restore lumbosacral stability. The aim of this study was to evaluate the accuracy of 3D printing technology for precise osteotomy during total sacrectomy.
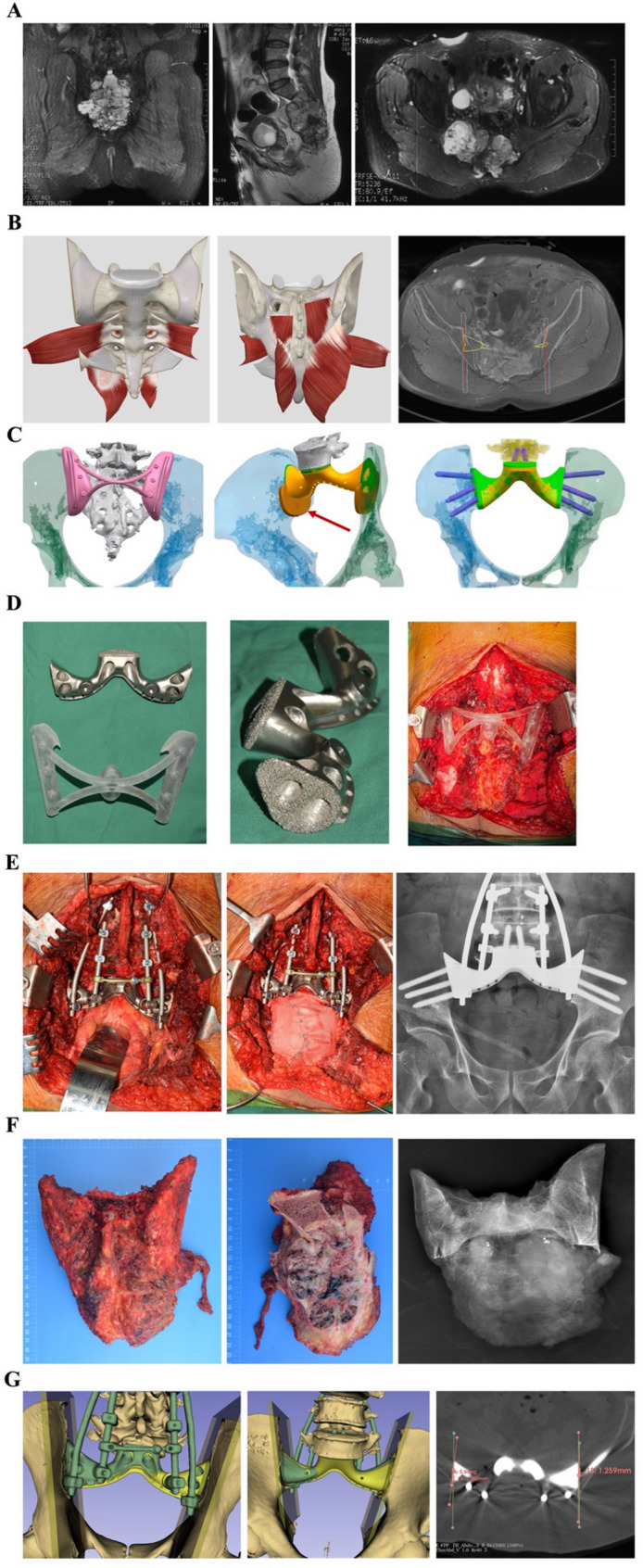
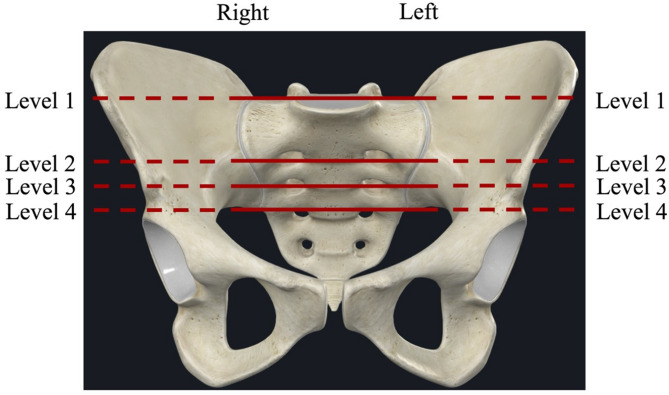
Methods: Nine patients with primary malignant tumors of the sacrum who underwent total sacrectomy at our center were enrolled. Osteotomy was planned based on preoperative imaging (CT, MRI). Generally, an additional 8-10 mm margin beyond the tumor was determined by the fusion of MR and CT images. Patient-specific surgical jigs and 3D-printed sacral endoprostheses were then designed based on the planned osteotomy planes. Pre- and postoperative 3D models of the lumbosacral and pelvic regions were constructed using the fiducial registration model of 3D slicer software 5.1.0. Postoperative CT scans were compared with the planned osteomy planes based on preoperative CT scans, in order to evaluate the accuracy of the osteotomy and endoprosthetic reconstruction. For each patient, four levels of osteotomy planes were chosen, including the upper edge of the sacroiliac (SI) joint, the S1 and S2 foramen levels, and the caudal edge of the SI joint, for analyzing position and angular deviations between the preoperative plan and actual osteotomy along with the endoprosthesis position.
Results: Pathological diagnoses included four cases of osteosarcoma, four cases of chordoma, and one case of Ewing sarcoma. All osteotomies in nine patients achieved R0 resection, as verified pathologically. An average angular deviation of 4.27° (interquartile range[IQR] 4.15) and an osteotomy position deviation of 4.00 mm (IQR 2.90) were observed. The mean angular deviations of the four levels were 3.50° (IQR 6.02), 3.86° (IQR 2.55), 4.81° (IQR 4.37), and 4.92° (IQR 3.27). The mean position deviations at the four levels were 3.15 mm (IQR 3.54), 3.55 mm (IQR 1.37), 4.26 mm (IQR 2.61), and 4.86 mm (IQR 3.93). No significant difference was found among the angular and position deviations at different levels. However, the proportions of individuals with position deviations > 2 mm and > 5 mm were significantly greater at the caudal end of the SI joint than at the upper end. All position deviations were within 8 mm. The average follow-up duration was 24.4 months. At the last follow-up, three patients experienced local recurrence, and one patient died of disease. All endoprostheses were in place without significant displacement. The mean Musculoskeletal Tumor Society scoring system (MSTS93) and MUD scores (function and sensation of lower limbs (M), urination and uriesthesia (U), and defecation and rectal sensation (D)) were 19.4 (16 to 24) and 16.3 (12 to 24), respectively.
Conclusion: Notably, 3D-printed patient-specific surgical jigs exhibit high accuracy of osteotomy and lead to optimal surgical margin and reconstruction in total sacrectomy. Effective and reliable reconstruction can be achieved with a custom-made 3D-printed endoprosthesis. The application of 3D printing technology using patient-specific surgical jigs and the custom-made 3D-printed implants exhibited high surgical accuracy in total sacrectomy, as evidenced by accuracy validation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


