Qiang Hu, Yuan Teng, Yuan Yuan, Guodong Gao, Bingyang Ji
{"title":"Effects of Ulinastatin on Inflammation Response and Lung Tissue Injury in Deep Hypothermic Circulatory Arrest.","authors":"Qiang Hu, Yuan Teng, Yuan Yuan, Guodong Gao, Bingyang Ji","doi":"10.1093/icvts/ivaf177","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Deep hypothermic circulatory arrest (DHCA) is known to trigger a systemic inflammatory response and ischaemia-reperfusion injury, leading to exacerbated lung dysfunction. Ulinastatin (UTI) is a commonly used anti-inflammatory drug in clinical settings, but its protective effects may vary depending on the timing and dosage.</p><p><strong>Methods: </strong>A rat model of DHCA was established, and 2 different doses of UTI (5/10 × 104 U/kg; low/high dose) were administered. We measured the levels of inflammatory factors using enzyme-linked immunosorbent assay kits and assessed the functional indicators of lung tissue injury. All rats (n = 18) underwent the standard cardiopulmonary bypass (CPB) procedure with DHCA.</p><p><strong>Results: </strong>Following rewarming, the levels of interleukin-6 (IL-6), IL-10, tumour necrosis factor (TNF)-α, and neutrophil elastase 2 (ELA-2) gradually increased in rats exposed to DHCA. Compared to the DHCA group, both the UTI groups exhibited significant reductions in IL-6 (DHCA vs DHCA+UTI-H, 8931.68 ± 650.31 vs 2498.05 ± 552.16), TNF-α (DHCA vs DHCA+UTI-H, 633.74 ± 74.53 vs 221.19 ± 31.63), and ELA-2 (DHCA vs DHCA+UTI-H, 4.94 ± 0.49 vs 3.29 ± 0.34), while remarkably increased the IL-10 (DHCA vs DHCA+UTI-H, 975.04 ± 110.33 vs 3081.27 ± 554.10) levels 4 hours after weaning from CPB (all P < 0.05). Interestingly, the high dose of UTI demonstrated a dose-dependent inhibition of inflammation. Meanwhile, we found that UTI contributed to maintain haemodynamic stability, improve tissue perfusion, and reduce hypoxia, as evidenced by elevated heart rate, blood pressure, haematocrit and oxygenation index, and decreased glucose and lactate. Reduced pathological changes in lung histopathology were also observed after UTI intervention, especially in 10 × 104 U/kg group.</p><p><strong>Conclusions: </strong>This study revealed that administration of low to high doses of UTI during DHCA could reduce the release of inflammatory factors, exert anti-inflammatory effects, and alleviate lung injury.</p>","PeriodicalId":73406,"journal":{"name":"Interdisciplinary cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12401673/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interdisciplinary cardiovascular and thoracic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/icvts/ivaf177","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Deep hypothermic circulatory arrest (DHCA) is known to trigger a systemic inflammatory response and ischaemia-reperfusion injury, leading to exacerbated lung dysfunction. Ulinastatin (UTI) is a commonly used anti-inflammatory drug in clinical settings, but its protective effects may vary depending on the timing and dosage.
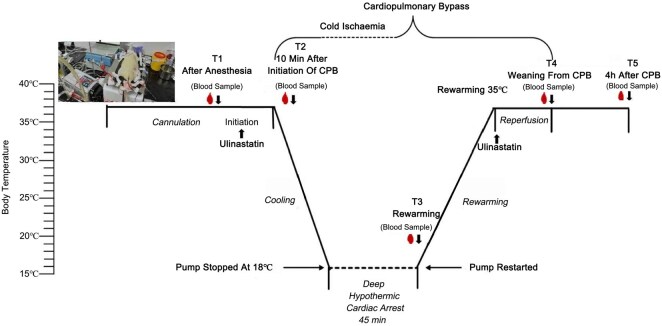
Methods: A rat model of DHCA was established, and 2 different doses of UTI (5/10 × 104 U/kg; low/high dose) were administered. We measured the levels of inflammatory factors using enzyme-linked immunosorbent assay kits and assessed the functional indicators of lung tissue injury. All rats (n = 18) underwent the standard cardiopulmonary bypass (CPB) procedure with DHCA.
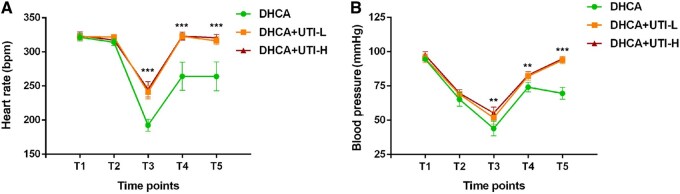
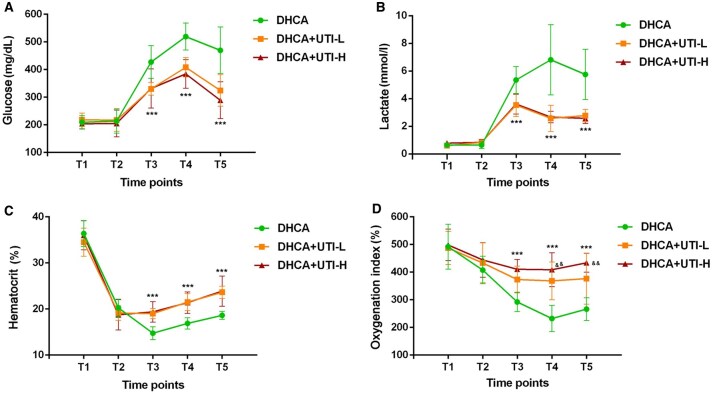
Results: Following rewarming, the levels of interleukin-6 (IL-6), IL-10, tumour necrosis factor (TNF)-α, and neutrophil elastase 2 (ELA-2) gradually increased in rats exposed to DHCA. Compared to the DHCA group, both the UTI groups exhibited significant reductions in IL-6 (DHCA vs DHCA+UTI-H, 8931.68 ± 650.31 vs 2498.05 ± 552.16), TNF-α (DHCA vs DHCA+UTI-H, 633.74 ± 74.53 vs 221.19 ± 31.63), and ELA-2 (DHCA vs DHCA+UTI-H, 4.94 ± 0.49 vs 3.29 ± 0.34), while remarkably increased the IL-10 (DHCA vs DHCA+UTI-H, 975.04 ± 110.33 vs 3081.27 ± 554.10) levels 4 hours after weaning from CPB (all P < 0.05). Interestingly, the high dose of UTI demonstrated a dose-dependent inhibition of inflammation. Meanwhile, we found that UTI contributed to maintain haemodynamic stability, improve tissue perfusion, and reduce hypoxia, as evidenced by elevated heart rate, blood pressure, haematocrit and oxygenation index, and decreased glucose and lactate. Reduced pathological changes in lung histopathology were also observed after UTI intervention, especially in 10 × 104 U/kg group.
Conclusions: This study revealed that administration of low to high doses of UTI during DHCA could reduce the release of inflammatory factors, exert anti-inflammatory effects, and alleviate lung injury.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


