Robot-assisted supratrigonal cystectomy and augmentation cystoplasty for adult neurogenic lower urinary tract dysfunction: comparison of extracorporeal versus intracorporeal diversion.
Neha Sihra, Pierre Lecoanet, Alexandre Dubois, Juan Penafiel, Camille Haudebert, Charles Mazeaud, Adil Mellouki, Juliette Hascoet, Younes Ahallal, Andrea Manunta, Imad Bentellis, Benoit Peyronnet
{"title":"Robot-assisted supratrigonal cystectomy and augmentation cystoplasty for adult neurogenic lower urinary tract dysfunction: comparison of extracorporeal versus intracorporeal diversion.","authors":"Neha Sihra, Pierre Lecoanet, Alexandre Dubois, Juan Penafiel, Camille Haudebert, Charles Mazeaud, Adil Mellouki, Juliette Hascoet, Younes Ahallal, Andrea Manunta, Imad Bentellis, Benoit Peyronnet","doi":"10.1177/17562872251359339","DOIUrl":null,"url":null,"abstract":"<p><p>We aim to explore the feasibility of robot-assisted supratrigonal cystectomy and augmentation cystoplasty (RA-SCAC) for the management of adult neurogenic lower urinary tract dysfunction and to compare the functional and surgical outcomes of an intracorporeal and extracorporeal approach. A retrospective review of all patients who underwent robot-assisted supratrigonal cystectomy and augmentation cystoplasty was performed. Data was collected on age, body mass index, American Society of Anaesthesiologists (ASA) score, type and duration of neurological disease, previous abdominal surgery and renal function. Bladder diary, urodynamics and validated symptom score results were recorded at baseline and repeated postoperatively. Intraoperative details included type of diversion, concomitant surgery, duration of surgery, blood loss and conversion to open. Postoperative surgical recovery was also reviewed. The primary endpoint was the rate of major postoperative complications defined as any complication Clavien-Dindo grade ≥3 occurring within the first 90 days postoperatively. There were 26 patients in total; 7 performed extracorporeally and 19 intracorporeally. Mean age was 41.5, mean BMI 24.4 and majority were ASA score 2 (61.5%). Twelve (46.1%) patients had spinal cord injury and 6 (23.1%) spina bifida. Seven (26.9%) had a concomitant procedure including bladder neck artificial urinary sphincter (AUS) insertion, bladder neck fascial sling or creation of a continent catheterisable channel. The surgical outcomes were analysed separately for those that had RA-SCAC only versus RA-SCAC with a concomitant procedure. The operative time was shorter in the intracorporeal group, and the length of stay was similar in both groups. The total number of major postoperative complications was low (n = 3; 11.5%). All urodynamic parameters significantly improved at 6 months in the intracorporeal group. Median number of urinary incontinence episodes per 24 h decreased significantly in both groups at 3 months but the continence status and ICIQ-UI SF demonstrated statistical significance in the intracorporeal group only. In conclusion, robot-assisted supratrigonal cystectomy and augmentation cystoplasty is feasible in adult neurological patients, favouring an intracorporeal approach.</p>","PeriodicalId":23010,"journal":{"name":"Therapeutic Advances in Urology","volume":"17 ","pages":"17562872251359339"},"PeriodicalIF":3.5000,"publicationDate":"2025-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12304641/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Urology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562872251359339","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
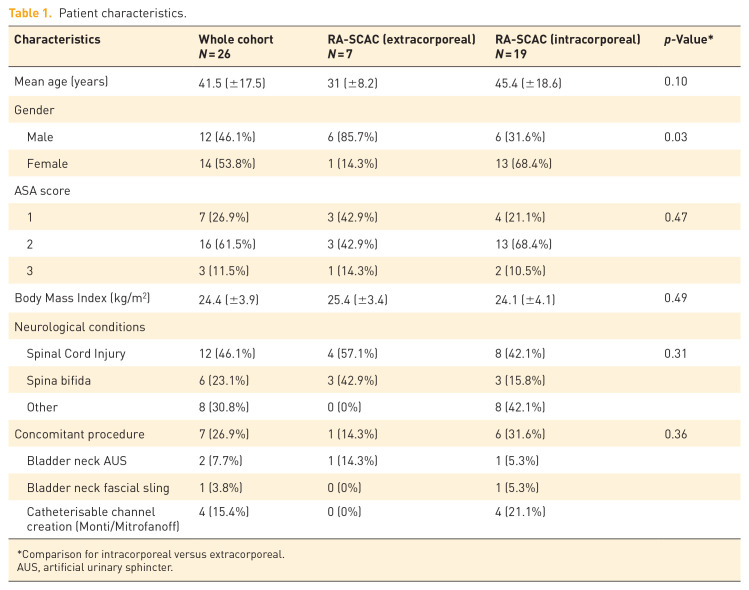
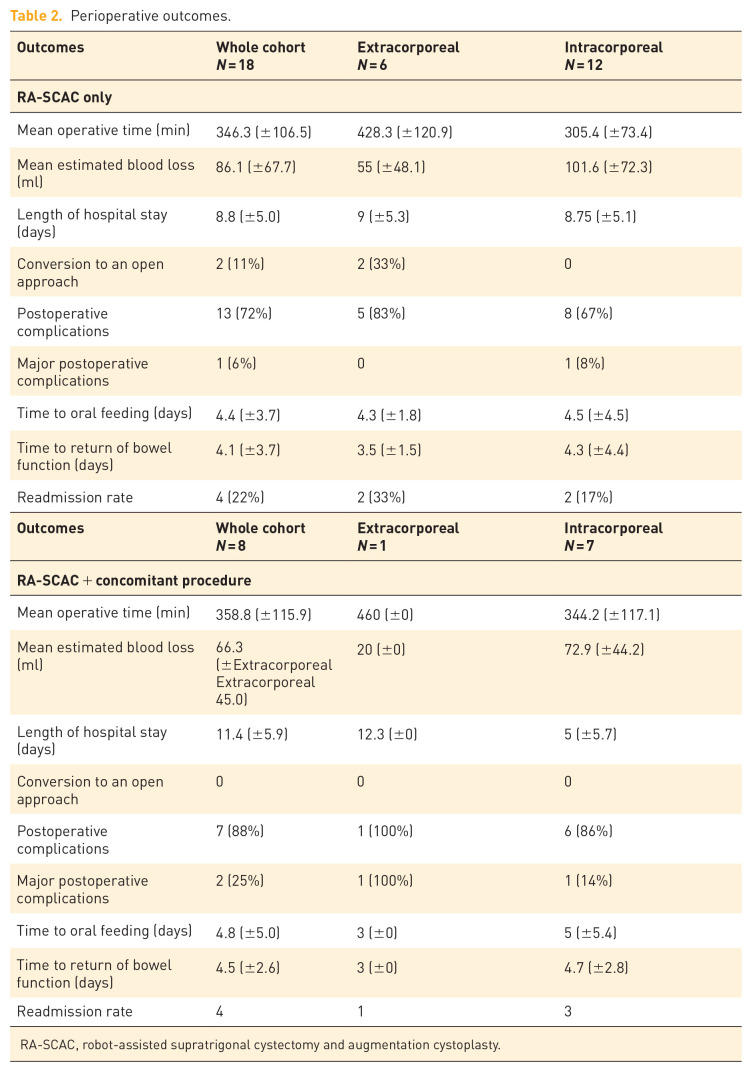
We aim to explore the feasibility of robot-assisted supratrigonal cystectomy and augmentation cystoplasty (RA-SCAC) for the management of adult neurogenic lower urinary tract dysfunction and to compare the functional and surgical outcomes of an intracorporeal and extracorporeal approach. A retrospective review of all patients who underwent robot-assisted supratrigonal cystectomy and augmentation cystoplasty was performed. Data was collected on age, body mass index, American Society of Anaesthesiologists (ASA) score, type and duration of neurological disease, previous abdominal surgery and renal function. Bladder diary, urodynamics and validated symptom score results were recorded at baseline and repeated postoperatively. Intraoperative details included type of diversion, concomitant surgery, duration of surgery, blood loss and conversion to open. Postoperative surgical recovery was also reviewed. The primary endpoint was the rate of major postoperative complications defined as any complication Clavien-Dindo grade ≥3 occurring within the first 90 days postoperatively. There were 26 patients in total; 7 performed extracorporeally and 19 intracorporeally. Mean age was 41.5, mean BMI 24.4 and majority were ASA score 2 (61.5%). Twelve (46.1%) patients had spinal cord injury and 6 (23.1%) spina bifida. Seven (26.9%) had a concomitant procedure including bladder neck artificial urinary sphincter (AUS) insertion, bladder neck fascial sling or creation of a continent catheterisable channel. The surgical outcomes were analysed separately for those that had RA-SCAC only versus RA-SCAC with a concomitant procedure. The operative time was shorter in the intracorporeal group, and the length of stay was similar in both groups. The total number of major postoperative complications was low (n = 3; 11.5%). All urodynamic parameters significantly improved at 6 months in the intracorporeal group. Median number of urinary incontinence episodes per 24 h decreased significantly in both groups at 3 months but the continence status and ICIQ-UI SF demonstrated statistical significance in the intracorporeal group only. In conclusion, robot-assisted supratrigonal cystectomy and augmentation cystoplasty is feasible in adult neurological patients, favouring an intracorporeal approach.
期刊介绍:
Therapeutic Advances in Urology delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of urology.
The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in urology, providing a forum in print and online for publishing the highest quality articles in this area. The editors welcome articles of current interest across all areas of urology, including treatment of urological disorders, with a focus on emerging pharmacological therapies.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


