Karol M. Pencina, David E. Leaf, Rodrigo J. Valderrabano, Sushrut S. Waikar, Tapan S. Mehta, Yili Valentine Shang, Nancy K. Latham, Tejossy John, Elena Volpi, Dahlene Fusco, Yusnie Memish-Beleva, Shobana Krishnamurthy, Siva Lavu, Salma Karmi, David J. Livingston, Shalender Bhasin
{"title":"Oral MIB-626 (β Nicotinamide Mononucleotide) Safely Raises Blood Nicotinamide Adenine Dinucleotide Levels in Hospitalized Patients With COVID-19 and Acute Kidney Injury: A Randomized Controlled Trial","authors":"Karol M. Pencina, David E. Leaf, Rodrigo J. Valderrabano, Sushrut S. Waikar, Tapan S. Mehta, Yili Valentine Shang, Nancy K. Latham, Tejossy John, Elena Volpi, Dahlene Fusco, Yusnie Memish-Beleva, Shobana Krishnamurthy, Siva Lavu, Salma Karmi, David J. Livingston, Shalender Bhasin","doi":"10.1096/fba.2025-00014","DOIUrl":null,"url":null,"abstract":"<p>Nicotinamide adenine dinucleotide (NAD<sup>+</sup>) plays an important role in the innate immune response and is depleted during SARS-CoV-2 infection due to increased turnover. It is unknown whether treatment with NAD<sup>+</sup> precursors can safely raise NAD<sup>+</sup> levels in patients with COVID-19. To determine whether MIB-626 (<i>β-</i>nicotinamide mononucleotide), an NAD<sup>+</sup> precursor, can safely increase blood NAD<sup>+</sup> levels and attenuate acute kidney injury (AKI) and inflammation in hospitalized patients with COVID-19, 42 adults, ≥ 18 years, hospitalized with COVID-19 and AKI, were randomized in a 3:2 ratio to MIB-626 1.0-g or placebo tablets twice daily for 14 days. Circulating NAD<sup>+</sup> and its metabolites, markers of AKI, inflammation, and disease severity, were assessed. MIB-626 treatment significantly but gradually raised blood NAD<sup>+</sup> levels to a peak between 5 to 14 days (16.0 ± 6.9, 25.5 ± 12.6, and 42.6 ± 25.6 μg/mL at baseline, days 5 and 14) and raised plasma concentrations of NAD<sup>+</sup> metabolites 1-methylnicotinamide, N-methyl, 2-pyridone, 4-carboxamide rapidly to a peak by day 3. Changes in serum creatinine, cystatin-C, and serum markers of AKI did not differ significantly between groups. Serum CRP, IL-6, and TNFα and indices of disease severity also did not differ between groups. MIB-626 treatment of patients with COVID-19 and AKI safely and substantially raised blood NAD<sup>+</sup> and plasma concentrations of NAD<sup>+</sup> metabolites. Markers of AKI, inflammation, and disease severity did not differ between groups, likely due to the slow rise in NAD<sup>+</sup> levels. Future studies should assess whether a rapid increase in NAD<sup>+</sup> by parenteral administration can attenuate disease severity and AKI.</p><p><b>Trial Registration:</b> ClinicalTrials.gov Identifier: NCT05038488</p>","PeriodicalId":12093,"journal":{"name":"FASEB bioAdvances","volume":"7 8","pages":""},"PeriodicalIF":2.0000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1096/fba.2025-00014","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"FASEB bioAdvances","FirstCategoryId":"1085","ListUrlMain":"https://faseb.onlinelibrary.wiley.com/doi/10.1096/fba.2025-00014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
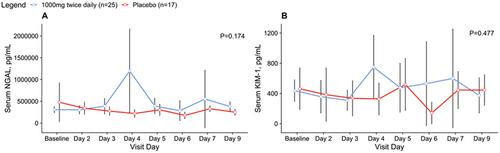
Nicotinamide adenine dinucleotide (NAD+) plays an important role in the innate immune response and is depleted during SARS-CoV-2 infection due to increased turnover. It is unknown whether treatment with NAD+ precursors can safely raise NAD+ levels in patients with COVID-19. To determine whether MIB-626 (β-nicotinamide mononucleotide), an NAD+ precursor, can safely increase blood NAD+ levels and attenuate acute kidney injury (AKI) and inflammation in hospitalized patients with COVID-19, 42 adults, ≥ 18 years, hospitalized with COVID-19 and AKI, were randomized in a 3:2 ratio to MIB-626 1.0-g or placebo tablets twice daily for 14 days. Circulating NAD+ and its metabolites, markers of AKI, inflammation, and disease severity, were assessed. MIB-626 treatment significantly but gradually raised blood NAD+ levels to a peak between 5 to 14 days (16.0 ± 6.9, 25.5 ± 12.6, and 42.6 ± 25.6 μg/mL at baseline, days 5 and 14) and raised plasma concentrations of NAD+ metabolites 1-methylnicotinamide, N-methyl, 2-pyridone, 4-carboxamide rapidly to a peak by day 3. Changes in serum creatinine, cystatin-C, and serum markers of AKI did not differ significantly between groups. Serum CRP, IL-6, and TNFα and indices of disease severity also did not differ between groups. MIB-626 treatment of patients with COVID-19 and AKI safely and substantially raised blood NAD+ and plasma concentrations of NAD+ metabolites. Markers of AKI, inflammation, and disease severity did not differ between groups, likely due to the slow rise in NAD+ levels. Future studies should assess whether a rapid increase in NAD+ by parenteral administration can attenuate disease severity and AKI.




 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


