Taha Benatiya Andaloussi, Mohamed Bouqes, Naouar Ouattassi, Mohamed Afellah, Mohammed Ridal, Najib Benmansour, Zouheir Zaki, Abdellatif Oudidi, Mohamed Noureddine El Amine El Alami
{"title":"Diagnosis and management of bilateral and multiple semicircular canal dehiscence: a case report.","authors":"Taha Benatiya Andaloussi, Mohamed Bouqes, Naouar Ouattassi, Mohamed Afellah, Mohammed Ridal, Najib Benmansour, Zouheir Zaki, Abdellatif Oudidi, Mohamed Noureddine El Amine El Alami","doi":"10.11604/pamj.2025.51.12.47421","DOIUrl":null,"url":null,"abstract":"<p><p>Semicircular canal dehiscence (SCCD) is a rare inner ear disease caused by an anatomical defect in the bony covering of the semicircular canal (SCC). This condition most commonly affects the superior semicircular canal, and less frequently involves multiple canals in one or both ears. Although the clinical and physiological features of a single SCCD are well known, there are only a few reported cases of multiple semicircular canal dehiscences. Thus, their clinical and physiological characteristics require further investigation. We present the case of a 59-year-old male patient of Moroccan ethnicity who presented with chronic imbalance and mild dizziness, induced by loud noises. As a dentist, he experienced extreme difficulty while drilling his patients' teeth, exhibiting nausea, tachycardia, and sweating. Clinical oto-vestibular and neurological examinations, tonal audiometry, and videonystagmography (VNG) revealed peripheral vestibular syndrome. Bilateral multiple SCCD was subsequently confirmed using high-resolution computed tomography imaging of the temporal bone. The clinical manifestations in this case were primarily neurovegetative symptoms of vestibular dysfunction. Functional assessments revealed vibratory-induced down-beating nystagmus and left preponderance on caloric testing. Computed tomography (CT) imaging confirmed dehiscence in the posterior and superior semicircular canals on the right side, and posterior semicircular canal dehiscence on the left side.</p>","PeriodicalId":48190,"journal":{"name":"Pan African Medical Journal","volume":"51 ","pages":"12"},"PeriodicalIF":1.0000,"publicationDate":"2025-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12296646/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pan African Medical Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.11604/pamj.2025.51.12.47421","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
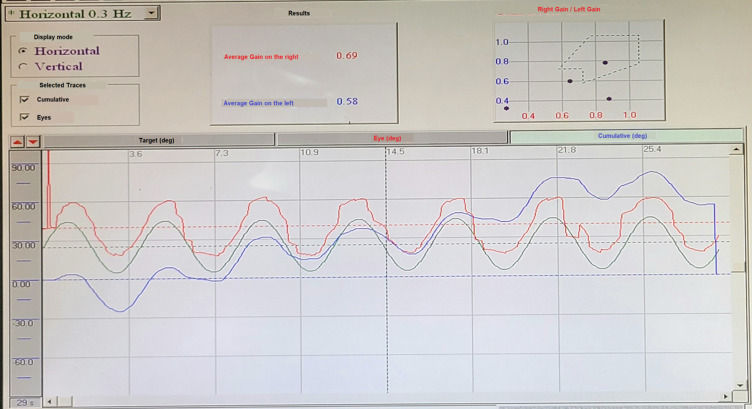
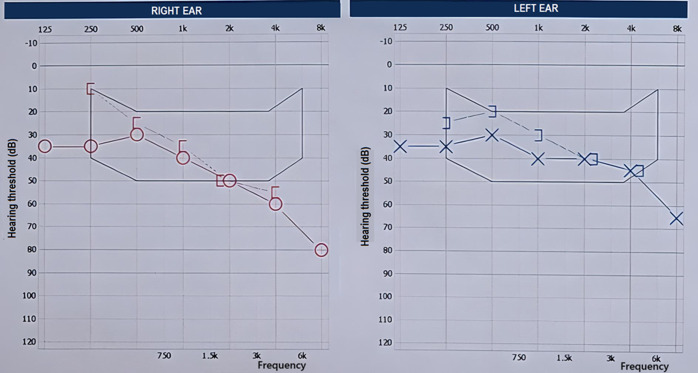
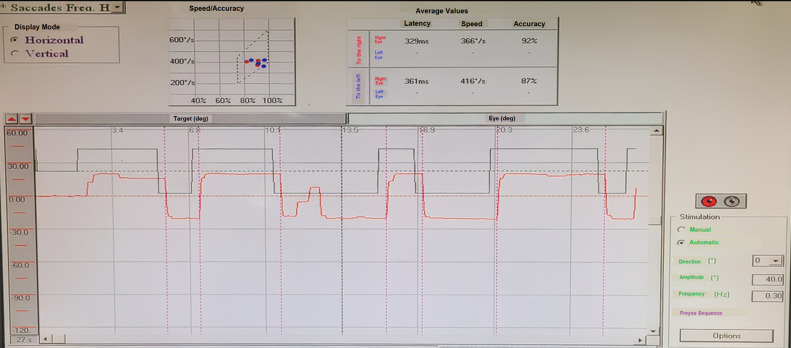
Semicircular canal dehiscence (SCCD) is a rare inner ear disease caused by an anatomical defect in the bony covering of the semicircular canal (SCC). This condition most commonly affects the superior semicircular canal, and less frequently involves multiple canals in one or both ears. Although the clinical and physiological features of a single SCCD are well known, there are only a few reported cases of multiple semicircular canal dehiscences. Thus, their clinical and physiological characteristics require further investigation. We present the case of a 59-year-old male patient of Moroccan ethnicity who presented with chronic imbalance and mild dizziness, induced by loud noises. As a dentist, he experienced extreme difficulty while drilling his patients' teeth, exhibiting nausea, tachycardia, and sweating. Clinical oto-vestibular and neurological examinations, tonal audiometry, and videonystagmography (VNG) revealed peripheral vestibular syndrome. Bilateral multiple SCCD was subsequently confirmed using high-resolution computed tomography imaging of the temporal bone. The clinical manifestations in this case were primarily neurovegetative symptoms of vestibular dysfunction. Functional assessments revealed vibratory-induced down-beating nystagmus and left preponderance on caloric testing. Computed tomography (CT) imaging confirmed dehiscence in the posterior and superior semicircular canals on the right side, and posterior semicircular canal dehiscence on the left side.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


