David J Horne, Jerry S Zifodya, Adrienne E Shapiro, Elizabeth Chandler Church, Jonah S Kreniske, Alexander W Kay, Katie Scandrett, Karen R Steingart, Yemisi Takwoingi
{"title":"Xpert MTB/RIF Ultra assay for pulmonary tuberculosis and rifampicin resistance in adults and adolescents.","authors":"David J Horne, Jerry S Zifodya, Adrienne E Shapiro, Elizabeth Chandler Church, Jonah S Kreniske, Alexander W Kay, Katie Scandrett, Karen R Steingart, Yemisi Takwoingi","doi":"10.1002/14651858.CD009593.pub6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Xpert MTB/RIF Ultra (Xpert Ultra) is a molecular World Health Organization (WHO)-recommended rapid diagnostic test that simultaneously detects tuberculosis and rifampicin resistance. This review updates a comparative accuracy Cochrane review of Xpert MTB/RIF and Xpert Ultra as Xpert Ultra has replaced Xpert MTB/RIF.</p><p><strong>Objectives: </strong>To determine the diagnostic accuracy of Xpert MTB/RIF Ultra (Xpert Ultra) for detecting pulmonary tuberculosis and rifampicin resistance in adults and adolescents with presumptive tuberculosis based on signs or symptoms or with an abnormal chest x-ray suggestive of tuberculosis.</p><p><strong>Search methods: </strong>We searched seven databases including CENTRAL, MEDLINE, and Embase, plus two trial registers (ClinicalTrials.gov and the WHO ICTRP) to 16 October 2023 without language restrictions. A WHO Public Call for ongoing and unpublished studies was made between 30 November 2023 and 15 February 2024.</p><p><strong>Selection criteria: </strong>We included cross-sectional studies, cohort studies, and randomised controlled trials that provided data on the diagnostic accuracy of Xpert Ultra using respiratory specimens in adolescents (aged 10 to 14 years) and adults (aged 15 years and older) with presumptive pulmonary tuberculosis. For pulmonary tuberculosis detection, the reference standards were culture and a composite reference standard. For rifampicin resistance, the reference standards were culture-based phenotypic drug susceptibility testing with or without whole genome sequencing.</p><p><strong>Data collection and analysis: </strong>Two review authors independently extracted data using a standardised form. We assessed risk of bias using QUADAS-2. We performed meta-analyses using a bivariate model to produce summary sensitivities and specificities, separately for pulmonary tuberculosis detection and rifampicin resistance detection. We performed subgroup analyses by smear status, HIV status, and history of tuberculosis. We summarised Xpert Ultra trace-positive results.</p><p><strong>Main results: </strong>Pulmonary tuberculosis detection For detection of pulmonary tuberculosis, Xpert Ultra summary sensitivity and specificity against culture were 90.7% (95% confidence interval (CI) 88.2 to 92.7) and 94.8% (95% CI 92.8 to 96.3) (32 studies, 12,529 participants; high-certainty evidence). Most studies had low risk of bias in all QUADAS-2 domains. If the point estimates for Xpert Ultra are applied to a hypothetical cohort of 1000 people, where 100 of those presenting with symptoms have pulmonary tuberculosis, Xpert Ultra will miss nine cases. The number of people wrongly diagnosed with pulmonary tuberculosis would be 47. In people living with HIV, Xpert Ultra summary sensitivity and specificity were 87.7% (82.0 to 91.7) and 95.3% (92.2 to 97.2) (11 studies, 1164 participants). Amongst people with smear-negative, culture-positive pulmonary tuberculosis, Xpert Ultra summary sensitivity and specificity were 80.7% (75.4 to 85.0) and 94.0% (91.3 to 95.9) (16 studies, 6460 participants). In people with a history of tuberculosis, Xpert Ultra summary sensitivity and specificity were 84.8% (78.2 to 89.7) and 86.2% (78.9 to 91.3) (9 studies, 809 participants). The proportion of Ultra trace-positive results that were true positives compared to the microbiological reference standard was 38.8%. Reclassifying trace-positive results as Xpert Ultra-negative led to a reduction in sensitivity and modest increase in specificity. Rifampicin resistance detection For detection of rifampicin resistance, Xpert Ultra summary sensitivity and specificity were 95.8% (93.2 to 97.4) and 98.3% (97.0 to 99.0) (10 studies, 1644 participants; high-certainty evidence). Most studies had low risk of bias in all QUADAS-2 domains. If the point estimates for Xpert Ultra are applied to a hypothetical cohort of 1000 people, where 100 of those presenting with symptoms have rifampicin resistance, Xpert Ultra will miss four cases. The number of people wrongly diagnosed with rifampicin resistance would be 16 out of the 900 who do not have rifampicin resistance. Xpert Ultra performed similarly, for rifampicin resistance, in people with smear-positive and smear-negative tuberculosis.</p><p><strong>Authors' conclusions: </strong>Xpert Ultra has high sensitivity and specificity for detection of pulmonary tuberculosis rifampicin resistance. Xpert Ultra for the detection of pulmonary tuberculosis has lower sensitivity in people with smear-negative/culture-positive tuberculosis and lower sensitivity and specificity in people with a history of tuberculosis. Xpert Ultra trace-positive results were common. Strengths of this review include the approach to identifying relevant studies, the number of studies and participants included in this systematic review, and that most studies were at low risk of bias. The small number of studies (six) and participants who were adolescents is a limitation to our accuracy estimates in this age group. Xpert Ultra testing provides accurate results and can allow rapid initiation of treatment for rifampicin-resistant and multiple-drug-resistant tuberculosis.</p><p><strong>Funding: </strong>The WHO supported this systematic review. Liverpool School of Tropical Medicine hosted the Cochrane Infectious Diseases Group (CIDG) editorial base, which supported the authors in the development of this review update. The Foreign, Commonwealth and Development Office funded the CIDG.</p><p><strong>Registration: </strong>Generic protocol available on Open Science Framework via https://osf.io/26wg7/wiki/home/. Previous protocol and review versions available via DOI 10.1002/14651858.CD009593 and DOI 10.1002/14651858.CD009593.pub5.</p>","PeriodicalId":10473,"journal":{"name":"Cochrane Database of Systematic Reviews","volume":"7 ","pages":"CD009593"},"PeriodicalIF":8.8000,"publicationDate":"2025-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12305759/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cochrane Database of Systematic Reviews","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/14651858.CD009593.pub6","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Xpert MTB/RIF Ultra (Xpert Ultra) is a molecular World Health Organization (WHO)-recommended rapid diagnostic test that simultaneously detects tuberculosis and rifampicin resistance. This review updates a comparative accuracy Cochrane review of Xpert MTB/RIF and Xpert Ultra as Xpert Ultra has replaced Xpert MTB/RIF.
Objectives: To determine the diagnostic accuracy of Xpert MTB/RIF Ultra (Xpert Ultra) for detecting pulmonary tuberculosis and rifampicin resistance in adults and adolescents with presumptive tuberculosis based on signs or symptoms or with an abnormal chest x-ray suggestive of tuberculosis.
Search methods: We searched seven databases including CENTRAL, MEDLINE, and Embase, plus two trial registers (ClinicalTrials.gov and the WHO ICTRP) to 16 October 2023 without language restrictions. A WHO Public Call for ongoing and unpublished studies was made between 30 November 2023 and 15 February 2024.
Selection criteria: We included cross-sectional studies, cohort studies, and randomised controlled trials that provided data on the diagnostic accuracy of Xpert Ultra using respiratory specimens in adolescents (aged 10 to 14 years) and adults (aged 15 years and older) with presumptive pulmonary tuberculosis. For pulmonary tuberculosis detection, the reference standards were culture and a composite reference standard. For rifampicin resistance, the reference standards were culture-based phenotypic drug susceptibility testing with or without whole genome sequencing.
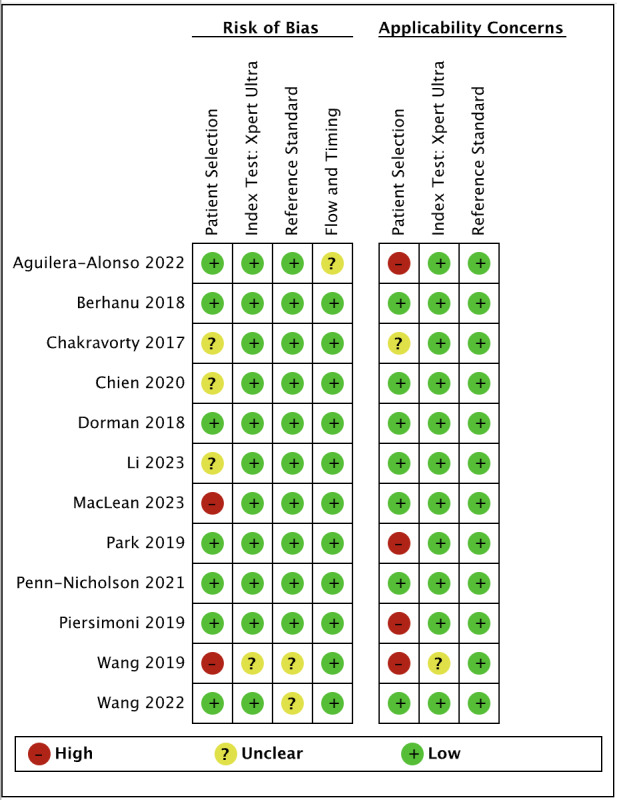
Data collection and analysis: Two review authors independently extracted data using a standardised form. We assessed risk of bias using QUADAS-2. We performed meta-analyses using a bivariate model to produce summary sensitivities and specificities, separately for pulmonary tuberculosis detection and rifampicin resistance detection. We performed subgroup analyses by smear status, HIV status, and history of tuberculosis. We summarised Xpert Ultra trace-positive results.
Main results: Pulmonary tuberculosis detection For detection of pulmonary tuberculosis, Xpert Ultra summary sensitivity and specificity against culture were 90.7% (95% confidence interval (CI) 88.2 to 92.7) and 94.8% (95% CI 92.8 to 96.3) (32 studies, 12,529 participants; high-certainty evidence). Most studies had low risk of bias in all QUADAS-2 domains. If the point estimates for Xpert Ultra are applied to a hypothetical cohort of 1000 people, where 100 of those presenting with symptoms have pulmonary tuberculosis, Xpert Ultra will miss nine cases. The number of people wrongly diagnosed with pulmonary tuberculosis would be 47. In people living with HIV, Xpert Ultra summary sensitivity and specificity were 87.7% (82.0 to 91.7) and 95.3% (92.2 to 97.2) (11 studies, 1164 participants). Amongst people with smear-negative, culture-positive pulmonary tuberculosis, Xpert Ultra summary sensitivity and specificity were 80.7% (75.4 to 85.0) and 94.0% (91.3 to 95.9) (16 studies, 6460 participants). In people with a history of tuberculosis, Xpert Ultra summary sensitivity and specificity were 84.8% (78.2 to 89.7) and 86.2% (78.9 to 91.3) (9 studies, 809 participants). The proportion of Ultra trace-positive results that were true positives compared to the microbiological reference standard was 38.8%. Reclassifying trace-positive results as Xpert Ultra-negative led to a reduction in sensitivity and modest increase in specificity. Rifampicin resistance detection For detection of rifampicin resistance, Xpert Ultra summary sensitivity and specificity were 95.8% (93.2 to 97.4) and 98.3% (97.0 to 99.0) (10 studies, 1644 participants; high-certainty evidence). Most studies had low risk of bias in all QUADAS-2 domains. If the point estimates for Xpert Ultra are applied to a hypothetical cohort of 1000 people, where 100 of those presenting with symptoms have rifampicin resistance, Xpert Ultra will miss four cases. The number of people wrongly diagnosed with rifampicin resistance would be 16 out of the 900 who do not have rifampicin resistance. Xpert Ultra performed similarly, for rifampicin resistance, in people with smear-positive and smear-negative tuberculosis.
Authors' conclusions: Xpert Ultra has high sensitivity and specificity for detection of pulmonary tuberculosis rifampicin resistance. Xpert Ultra for the detection of pulmonary tuberculosis has lower sensitivity in people with smear-negative/culture-positive tuberculosis and lower sensitivity and specificity in people with a history of tuberculosis. Xpert Ultra trace-positive results were common. Strengths of this review include the approach to identifying relevant studies, the number of studies and participants included in this systematic review, and that most studies were at low risk of bias. The small number of studies (six) and participants who were adolescents is a limitation to our accuracy estimates in this age group. Xpert Ultra testing provides accurate results and can allow rapid initiation of treatment for rifampicin-resistant and multiple-drug-resistant tuberculosis.
Funding: The WHO supported this systematic review. Liverpool School of Tropical Medicine hosted the Cochrane Infectious Diseases Group (CIDG) editorial base, which supported the authors in the development of this review update. The Foreign, Commonwealth and Development Office funded the CIDG.
Registration: Generic protocol available on Open Science Framework via https://osf.io/26wg7/wiki/home/. Previous protocol and review versions available via DOI 10.1002/14651858.CD009593 and DOI 10.1002/14651858.CD009593.pub5.
期刊介绍:
The Cochrane Database of Systematic Reviews (CDSR) stands as the premier database for systematic reviews in healthcare. It comprises Cochrane Reviews, along with protocols for these reviews, editorials, and supplements. Owned and operated by Cochrane, a worldwide independent network of healthcare stakeholders, the CDSR (ISSN 1469-493X) encompasses a broad spectrum of health-related topics, including health services.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


