Diaphragmatic ultrasound-derived MV×DE: a novel predictor of postextubation adverse respiratory events in general anesthesia patients (observational study).
{"title":"Diaphragmatic ultrasound-derived MV×DE: a novel predictor of postextubation adverse respiratory events in general anesthesia patients (observational study).","authors":"Jing Huang, Yanzi Yi, Xiaotian Zhang, XiaoXiao Li, Zhouquan Wu","doi":"10.1186/s12890-025-03831-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study explored the potential of diaphragmatic ultrasonography in the postanaesthesia care unit (PACU) for predicting postextubation adverse respiratory events (PAREs) in patients recovering from general anaesthesia.--.</p><p><strong>Methods: </strong>This cohort study included 110 patients who underwent elective surgeries under general anaesthesia. During recovery before extubation, diaphragmatic function was monitored via ultrasound with pressure support ventilation on continuous positive airway pressure (PS/CPAP). Concurrent respiratory parameters (tidal volume, respiratory rate, and PEEP) were also recorded. Patients were categorized into PARE and nonadverse respiratory event groups based on postextubation outcomes. A composite metric, MV×DE, was calculated by multiplying minute ventilation (MV) by diaphragmatic excursion (DE). Independent predictors of PAREs were identified using multivariate logistic regression, and the diagnostic accuracy of each indicator for PAREs was assessed using ROC curve analysis.</p><p><strong>Results: </strong>The final cohort consisted of 106 participants under general anesthesia, divided into two subgroups based on postextubation outcomes. Analysis showed significant demographic differences between those with postextubation respiratory events (n = 33) and those without (n = 73). The PARE group was older (66.7 ± 16.6 vs. 56.1 ± 15.2 years, p < 0.001) and had a higher prevalence of ASA class III status (48.5% vs. 16.0%, p < 0.001). Diaphragm function indices also differed significantly; the PARE group had reduced diaphragmatic excursion (DE), lower diaphragmatic thickness fraction (DTF), and lower combined parameters (RR×DE and RR×DTF) (all p < 0.001). Multivariate logistic regression identified MV×DE during extubation as the strongest predictor of adverse respiratory outcomes in the PACU (p < 0.001). MV×DE demonstrated strong diagnostic performance with optimal discrimination at ≤ 0.65, showing superior predictive ability (AUROC = 0.874, 95% CI 0.801-0.947), with 78.8% sensitivity and 86.3% specificity for high-risk patients (p < 0.001).</p><p><strong>Conclusion: </strong>MV × DE represents a promising tool for predicting postextubation adverse respiratory events (PEREs) in patients under general anaesthesia in the postanaesthesia care unit (PACU). Additionally, in terms of predicting PAREs, MV × DE offers greater reliability than traditional diaphragm parameters alone do.</p>","PeriodicalId":9148,"journal":{"name":"BMC Pulmonary Medicine","volume":"25 1","pages":"354"},"PeriodicalIF":2.8000,"publicationDate":"2025-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12302765/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Pulmonary Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12890-025-03831-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This study explored the potential of diaphragmatic ultrasonography in the postanaesthesia care unit (PACU) for predicting postextubation adverse respiratory events (PAREs) in patients recovering from general anaesthesia.--.
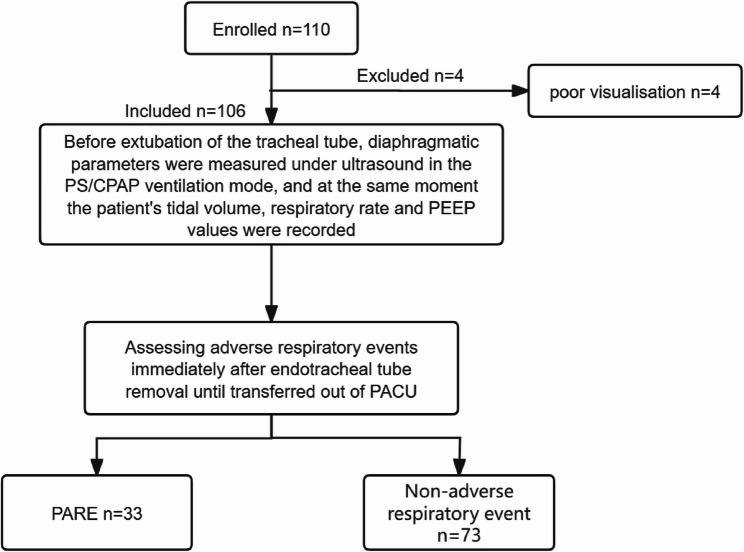
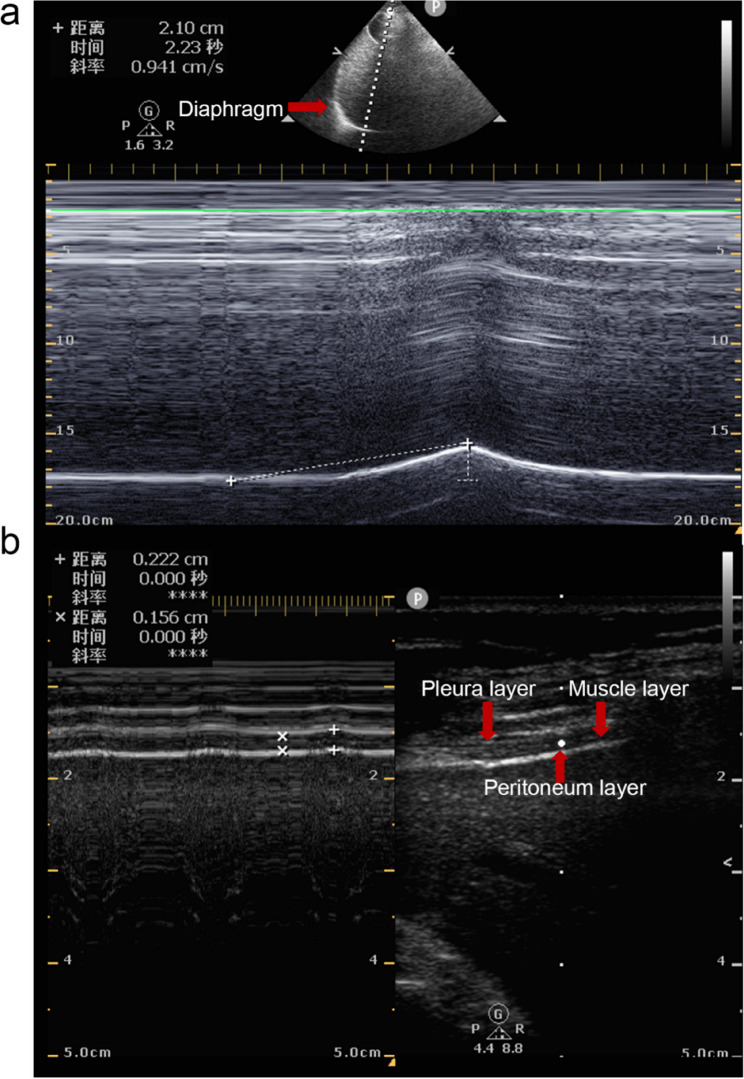
Methods: This cohort study included 110 patients who underwent elective surgeries under general anaesthesia. During recovery before extubation, diaphragmatic function was monitored via ultrasound with pressure support ventilation on continuous positive airway pressure (PS/CPAP). Concurrent respiratory parameters (tidal volume, respiratory rate, and PEEP) were also recorded. Patients were categorized into PARE and nonadverse respiratory event groups based on postextubation outcomes. A composite metric, MV×DE, was calculated by multiplying minute ventilation (MV) by diaphragmatic excursion (DE). Independent predictors of PAREs were identified using multivariate logistic regression, and the diagnostic accuracy of each indicator for PAREs was assessed using ROC curve analysis.
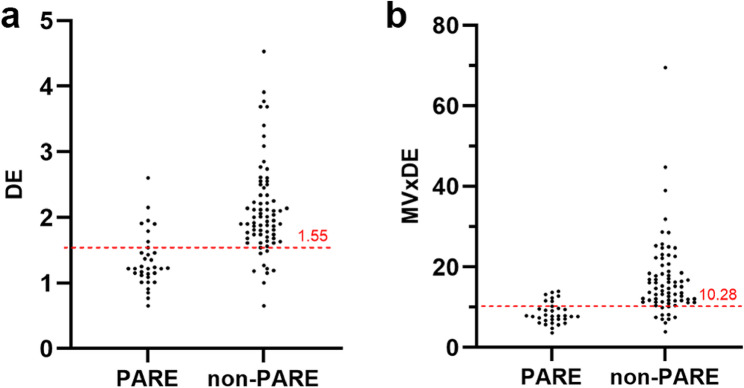
Results: The final cohort consisted of 106 participants under general anesthesia, divided into two subgroups based on postextubation outcomes. Analysis showed significant demographic differences between those with postextubation respiratory events (n = 33) and those without (n = 73). The PARE group was older (66.7 ± 16.6 vs. 56.1 ± 15.2 years, p < 0.001) and had a higher prevalence of ASA class III status (48.5% vs. 16.0%, p < 0.001). Diaphragm function indices also differed significantly; the PARE group had reduced diaphragmatic excursion (DE), lower diaphragmatic thickness fraction (DTF), and lower combined parameters (RR×DE and RR×DTF) (all p < 0.001). Multivariate logistic regression identified MV×DE during extubation as the strongest predictor of adverse respiratory outcomes in the PACU (p < 0.001). MV×DE demonstrated strong diagnostic performance with optimal discrimination at ≤ 0.65, showing superior predictive ability (AUROC = 0.874, 95% CI 0.801-0.947), with 78.8% sensitivity and 86.3% specificity for high-risk patients (p < 0.001).
Conclusion: MV × DE represents a promising tool for predicting postextubation adverse respiratory events (PEREs) in patients under general anaesthesia in the postanaesthesia care unit (PACU). Additionally, in terms of predicting PAREs, MV × DE offers greater reliability than traditional diaphragm parameters alone do.
期刊介绍:
BMC Pulmonary Medicine is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of pulmonary and associated disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


