{"title":"Real-Time Telemedical Oversight Improves Prehospital Stroke Metrics: A Five-Year Cohort Study.","authors":"Ponlawat Kanchayawong, Kasamon Aramvanitch, Chaiyaporn Yuksen, Satariya Trakulsrichai, Pungkava Sricharoen, Sureerat Suwatcharangkoon, Patcharaporn Sirintaranont, Jesada Keandoungchun, Promphet Nuanprom, Chetsadakon Jenpanitpong, Suthap Jaiboon","doi":"10.22037/aaemj.v13i1.2693","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>By enabling direct consultation with neurologists, Real-Time Telemedical Oversight (ReTMO) can facilitate rapid stroke assessment and decision-making. This study aimed to assess the efficacy of prehospital stroke management before and after ReTMO implementation.</p><p><strong>Methods: </strong><b>A</b> single-center retrospective before-and-after study was conducted at Ramathibodi Hospital, Bangkok, Thailand, from January 2020 to December 2024. In March 2022, a structured prehospital stroke protocol was integrated with the ReTMO system in this hospital. We evaluated its impact by comparing stroke patients transported by emergency medical services (EMS) before and after protocol implementation. Neurological outcomes at hospital discharge were analyzed using multivariable ordinal logistic regression. In contrast, door-to-treatment times in the emergency department (ED) and hospital length of stay were assessed using multivariable Gaussian regression.</p><p><strong>Results: </strong>The study included 91 prehospital stroke patients, with 36 in the pre-protocol group and 55 in the post-protocol group. Implementation of the structured prehospital stroke protocol was associated with a significant reduction in door-to-computed tomography (CT) scan time by 10.47 (95% confidence interval (CI): -17.62 to -3.3) minutes and door-to-laboratory result time by 15.90 (95% CI: -30.48 to -1.33) minutes. Additionally, adjusted ordinal logistic regression analysis demonstrated a significant improvement in neurological outcomes at hospital discharge (odds ratio (OR) = 0.14, 95% CI: 0.02-0.99, P = 0.049). However, reductions in ED stroke treatment time and hospital length of stay were not statistically significant.</p><p><strong>Conclusions: </strong>Implementing ReTMO alongside a structured prehospital stroke protocol significantly reduced in-hospital delays in door-to-CT and door-to-laboratory result times while also improving neurological outcomes at hospital discharge.</p>","PeriodicalId":8146,"journal":{"name":"Archives of Academic Emergency Medicine","volume":"13 1","pages":"e57"},"PeriodicalIF":2.0000,"publicationDate":"2025-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12303409/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Academic Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22037/aaemj.v13i1.2693","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: By enabling direct consultation with neurologists, Real-Time Telemedical Oversight (ReTMO) can facilitate rapid stroke assessment and decision-making. This study aimed to assess the efficacy of prehospital stroke management before and after ReTMO implementation.
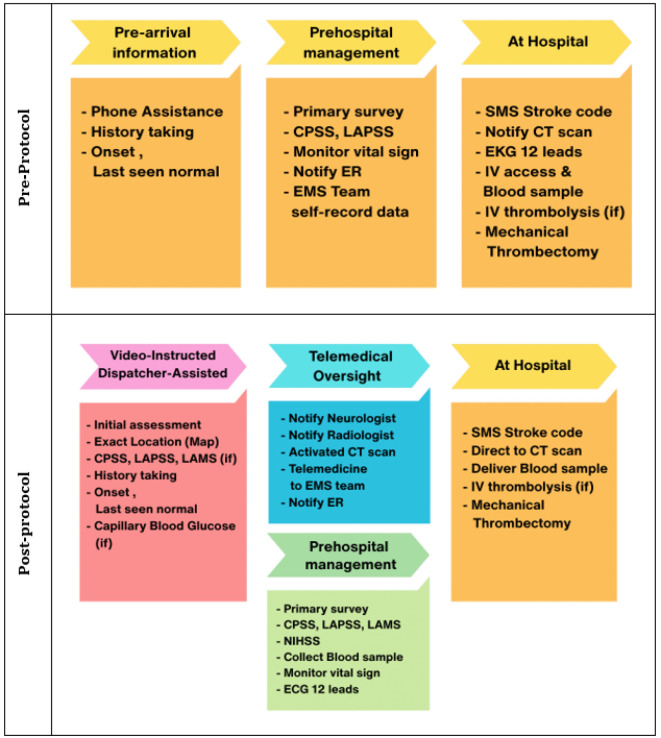
Methods: A single-center retrospective before-and-after study was conducted at Ramathibodi Hospital, Bangkok, Thailand, from January 2020 to December 2024. In March 2022, a structured prehospital stroke protocol was integrated with the ReTMO system in this hospital. We evaluated its impact by comparing stroke patients transported by emergency medical services (EMS) before and after protocol implementation. Neurological outcomes at hospital discharge were analyzed using multivariable ordinal logistic regression. In contrast, door-to-treatment times in the emergency department (ED) and hospital length of stay were assessed using multivariable Gaussian regression.
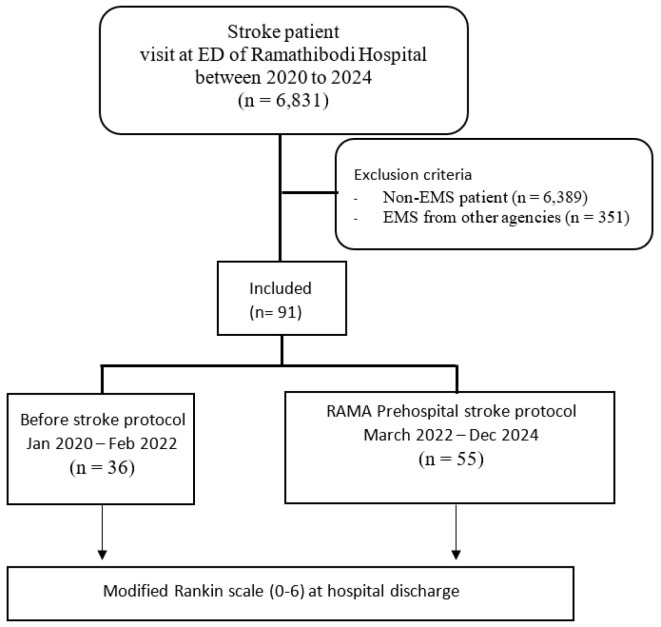
Results: The study included 91 prehospital stroke patients, with 36 in the pre-protocol group and 55 in the post-protocol group. Implementation of the structured prehospital stroke protocol was associated with a significant reduction in door-to-computed tomography (CT) scan time by 10.47 (95% confidence interval (CI): -17.62 to -3.3) minutes and door-to-laboratory result time by 15.90 (95% CI: -30.48 to -1.33) minutes. Additionally, adjusted ordinal logistic regression analysis demonstrated a significant improvement in neurological outcomes at hospital discharge (odds ratio (OR) = 0.14, 95% CI: 0.02-0.99, P = 0.049). However, reductions in ED stroke treatment time and hospital length of stay were not statistically significant.
Conclusions: Implementing ReTMO alongside a structured prehospital stroke protocol significantly reduced in-hospital delays in door-to-CT and door-to-laboratory result times while also improving neurological outcomes at hospital discharge.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


