{"title":"Different Resuscitation Termination Criteria for Out of Hospital Cardiac Arrest; A Prognostic Accuracy Study.","authors":"Phatcha Termkijwanich, Pitsucha Sanguanwit, Chaiyaporn Yuksen, Satariya Trakulsrichai, Pungkava Sricharoen","doi":"10.22037/aaemj.v13i1.2656","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Termination of resuscitation (TOR) rules in out of hospital cardiac arrest (OHCA) varies across different healthcare settings and populations. This study aimed to externally validate ten TOR rules for predicting death before hospital admission among OHCA patients.</p><p><strong>Methods: </strong>A retrospective prognostic accuracy study analyzed 379 non-trauma OHCA patients (≥18 years) in Bangkok who were either treated by the emergency medical services (EMS) of Ramathibodi Hospital or transported to Ramathibodi's emergency department by another EMS provider (January 2010 - March 2023). The predictive performance of ten TOR rules (AHA-BLS, AHA-ALS, Korean Cardiac Arrest Research Consortium (KoCARC) rules I, II, and III, Goto's rule, Shihabashi's rule, the New Model I, Helsinki's, and Petrie's rule) in predicting death before hospital admission as well as false positive rates (FPRs) of rules at various resuscitation times were calculated and reported with 95% confidence interval (CI).</p><p><strong>Results: </strong>Among 379 OHCA patients, 308 (81.27%) died before hospital admission and 71 (18.73%) survived to discharge. The New model I demonstrated the most conservative predictive performance with sensitivity of 96.7% (95% CI: 93.0-98.8), NPV of 91.5% (95% CI: 82.5-96.8), and area under the curve (AUC) of 0.74 (95% CI: 0.70-0.79). The KoCARC III showed FPR of 2.8%. Based on the initial presenting criteria, the FPR varied at different resuscitation time points, with increasing FPR over 30 minutes. Among all rules, Helsinki's and AHA-BLS showed the highest FPRs (1.14 - 21.13 and 1.14 - 23.94, respectively) while the KoCARC TOR rules III demonstrated the most conservative consistency in maintaining a low FPR (0-2.82%) throughout time.</p><p><strong>Conclusion: </strong>The KoCARC III demonstrated relatively high safety for TOR decisions in Bangkok's OHCA population, with the lowest FPR, and high sensitivity and NPV. TOR rules showed higher FPRs compared to previous studies. These findings should be interpreted with caution due to the retrospective design, potential selection bias, and EMS protocol changes over the 10-year study period.</p>","PeriodicalId":8146,"journal":{"name":"Archives of Academic Emergency Medicine","volume":"13 1","pages":"e59"},"PeriodicalIF":2.0000,"publicationDate":"2025-06-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12303412/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Academic Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22037/aaemj.v13i1.2656","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Termination of resuscitation (TOR) rules in out of hospital cardiac arrest (OHCA) varies across different healthcare settings and populations. This study aimed to externally validate ten TOR rules for predicting death before hospital admission among OHCA patients.
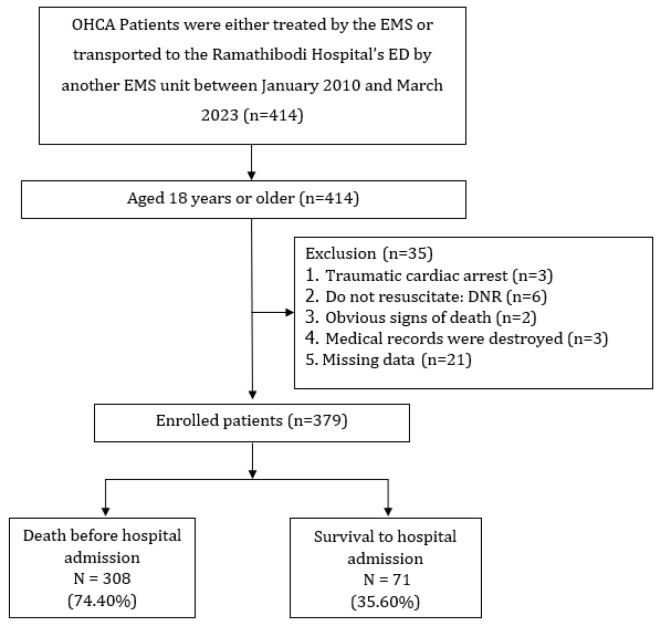
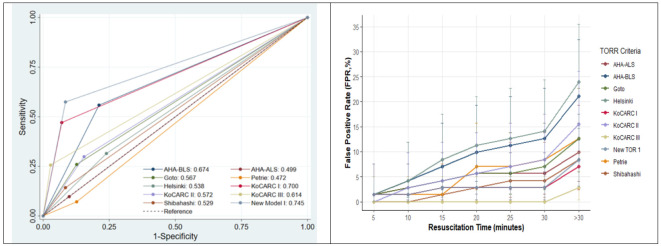
Methods: A retrospective prognostic accuracy study analyzed 379 non-trauma OHCA patients (≥18 years) in Bangkok who were either treated by the emergency medical services (EMS) of Ramathibodi Hospital or transported to Ramathibodi's emergency department by another EMS provider (January 2010 - March 2023). The predictive performance of ten TOR rules (AHA-BLS, AHA-ALS, Korean Cardiac Arrest Research Consortium (KoCARC) rules I, II, and III, Goto's rule, Shihabashi's rule, the New Model I, Helsinki's, and Petrie's rule) in predicting death before hospital admission as well as false positive rates (FPRs) of rules at various resuscitation times were calculated and reported with 95% confidence interval (CI).
Results: Among 379 OHCA patients, 308 (81.27%) died before hospital admission and 71 (18.73%) survived to discharge. The New model I demonstrated the most conservative predictive performance with sensitivity of 96.7% (95% CI: 93.0-98.8), NPV of 91.5% (95% CI: 82.5-96.8), and area under the curve (AUC) of 0.74 (95% CI: 0.70-0.79). The KoCARC III showed FPR of 2.8%. Based on the initial presenting criteria, the FPR varied at different resuscitation time points, with increasing FPR over 30 minutes. Among all rules, Helsinki's and AHA-BLS showed the highest FPRs (1.14 - 21.13 and 1.14 - 23.94, respectively) while the KoCARC TOR rules III demonstrated the most conservative consistency in maintaining a low FPR (0-2.82%) throughout time.
Conclusion: The KoCARC III demonstrated relatively high safety for TOR decisions in Bangkok's OHCA population, with the lowest FPR, and high sensitivity and NPV. TOR rules showed higher FPRs compared to previous studies. These findings should be interpreted with caution due to the retrospective design, potential selection bias, and EMS protocol changes over the 10-year study period.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


