{"title":"Calculation of Sensitivity and Specificity from Partial Data for Meta-Analyses: Introducing Some Practical Methods.","authors":"Reihanesadat Khatami, Mohammadsadegh Faghihi, Hannanesadat Khatami, Mahmoud Yousefifard, Seyedhesamoddin Khatami","doi":"10.22037/aaemj.v13i1.2678","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Meta-analyses of diagnostic/prognostic studies for calculating the pooled sensitivity and specificity require true positive (TP), true negative (TN), false positive (FP), and false negative (FN) counts. However, few studies report these values directly. This study aimed to consolidate practical methods to reconstruct sensitivity and specificity from minimal data.</p><p><strong>Methods: </strong>Our framework addresses three main situations: (1) algebraic rearrangements to compute specificity given partial metrics; (2) digitization of receiver operating characteristic (ROC) curves to obtain threshold-specific sensitivity and specificity; and (3) application of the binormal model when only AUC and prevalence are available. We tested these methods on a dataset related to mortality prediction in myocardial infarction (MI) using machine learning models, assessing how well they reconstructed sensitivity and specificity.</p><p><strong>Results: </strong>Algebraic formulas and ROC digitization yielded reliable estimates when partial metrics or graphical curves were sufficiently detailed. However, the binormal model, which assumes equal variances, showed noticeable inaccuracies, especially for sensitivity. Linear regression analyses indicated that higher prevalence and higher AUC reduced estimation errors.</p><p><strong>Conclusion: </strong>These methods offer practical alternatives for reconstructing diagnostic accuracy measures when data are incomplete. Relying solely on AUC-based estimations may introduce substantial bias, particularly in low-prevalence contexts. We recommend that primary studies report threshold-specific sensitivity and specificity to support more accurate meta-analytic estimations.</p>","PeriodicalId":8146,"journal":{"name":"Archives of Academic Emergency Medicine","volume":"13 1","pages":"e56"},"PeriodicalIF":2.0000,"publicationDate":"2025-07-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12303406/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Academic Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22037/aaemj.v13i1.2678","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Meta-analyses of diagnostic/prognostic studies for calculating the pooled sensitivity and specificity require true positive (TP), true negative (TN), false positive (FP), and false negative (FN) counts. However, few studies report these values directly. This study aimed to consolidate practical methods to reconstruct sensitivity and specificity from minimal data.
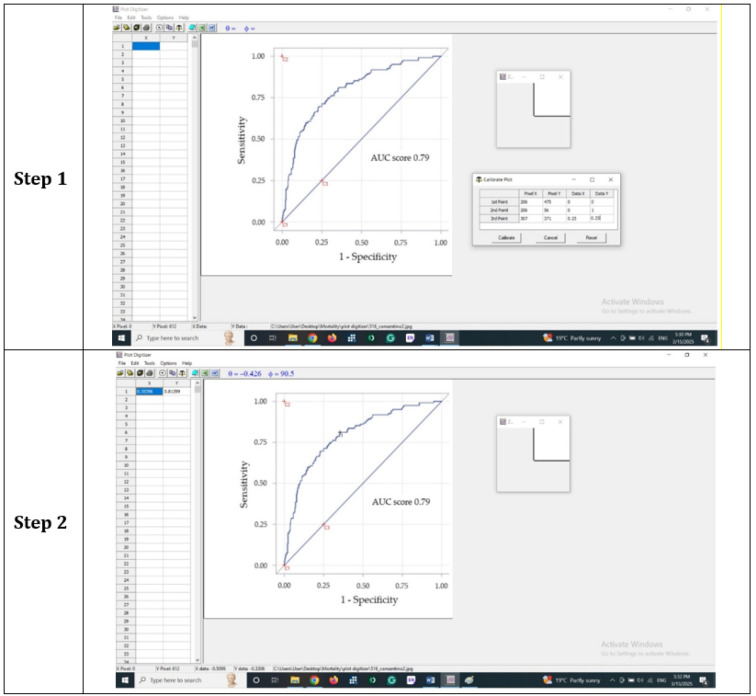
Methods: Our framework addresses three main situations: (1) algebraic rearrangements to compute specificity given partial metrics; (2) digitization of receiver operating characteristic (ROC) curves to obtain threshold-specific sensitivity and specificity; and (3) application of the binormal model when only AUC and prevalence are available. We tested these methods on a dataset related to mortality prediction in myocardial infarction (MI) using machine learning models, assessing how well they reconstructed sensitivity and specificity.
Results: Algebraic formulas and ROC digitization yielded reliable estimates when partial metrics or graphical curves were sufficiently detailed. However, the binormal model, which assumes equal variances, showed noticeable inaccuracies, especially for sensitivity. Linear regression analyses indicated that higher prevalence and higher AUC reduced estimation errors.
Conclusion: These methods offer practical alternatives for reconstructing diagnostic accuracy measures when data are incomplete. Relying solely on AUC-based estimations may introduce substantial bias, particularly in low-prevalence contexts. We recommend that primary studies report threshold-specific sensitivity and specificity to support more accurate meta-analytic estimations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


