Amany Faheem Omara, Alaa Mohammed Abo Hagar, Asmaa Fawzy Amer
{"title":"The Effect of Esmolol Versus Dexmedetomidine on Postoperative Pain Control in Endoscopic Sinus Surgery: A Randomized Trial.","authors":"Amany Faheem Omara, Alaa Mohammed Abo Hagar, Asmaa Fawzy Amer","doi":"10.5812/aapm-158065","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Functional endoscopic sinus surgery (FESS) is the cornerstone of treatment for nasal pathology.</p><p><strong>Objectives: </strong>This randomized study compares the ability of preoperative and intraoperative esmolol and dexmedetomidine to induce postoperative analgesia and sedation.</p><p><strong>Methods: </strong>Seventy ASA I and II patients, of either sex, scheduled for FESS, were divided into two groups: The esmolol group (group E) received an intravenous bolus dose of 0.5 mg/kg prior to the induction of anesthesia, followed by 0.05 mg/kg/min and stopped immediately upon extubation, while the dexmedetomidine group (group D) received 1 µg/kg of dexmedetomidine over 10 minutes, immediately before the induction of anesthesia, followed by a 0.5 µg/kg/hour infusion after induction and stopped immediately upon extubation. Mean arterial pressure and heart rate were monitored before induction, before and after intubation, and then every 5 to 30 minutes, as well as every 10 minutes until 90 minutes following the commencement of the IV medication infusion. The sedation level was assessed using the Ramsay sedation scale at 15, 30, and 60 minutes postoperatively. Pain scores were evaluated in the recovery room (on arrival and then 15 minutes, 30 minutes, and 1 hour later) and at 2 hours, 6 hours, 12 hours, and 24 hours. The length of the procedure, the degree of bleeding during the intervention, and the occurrence of any adverse effects were documented. Categorical data were summarized as counts and percentages and compared by the chi-square test. Continuous data were assessed for normality using the Shapiro-Wilk test. The Student's <i>t</i>-test was used for quantitative variables that are normally distributed, whereas the Mann-Whitney test was used for quantitative variables that are not.</p><p><strong>Results: </strong>According to our findings, both esmolol and dexmedetomidine were safe and beneficial in reducing blood loss during FESS, promoting optimal surgical field quality, and improving surgical field visibility. Dexmedetomidine was far more effective in providing postoperative sedation, reducing the need for opioids, and delaying the initial need for postoperative analgesia.</p><p><strong>Conclusions: </strong>It was discovered that esmolol and dexmedetomidine both provided superior surgical field, less nasal hemorrhage, and more successful results. Dexmedetomidine caused effective sedation and a reduced need for analgesics.</p>","PeriodicalId":7841,"journal":{"name":"Anesthesiology and Pain Medicine","volume":"15 3","pages":"e158065"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12297030/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesiology and Pain Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5812/aapm-158065","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/30 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Functional endoscopic sinus surgery (FESS) is the cornerstone of treatment for nasal pathology.
Objectives: This randomized study compares the ability of preoperative and intraoperative esmolol and dexmedetomidine to induce postoperative analgesia and sedation.
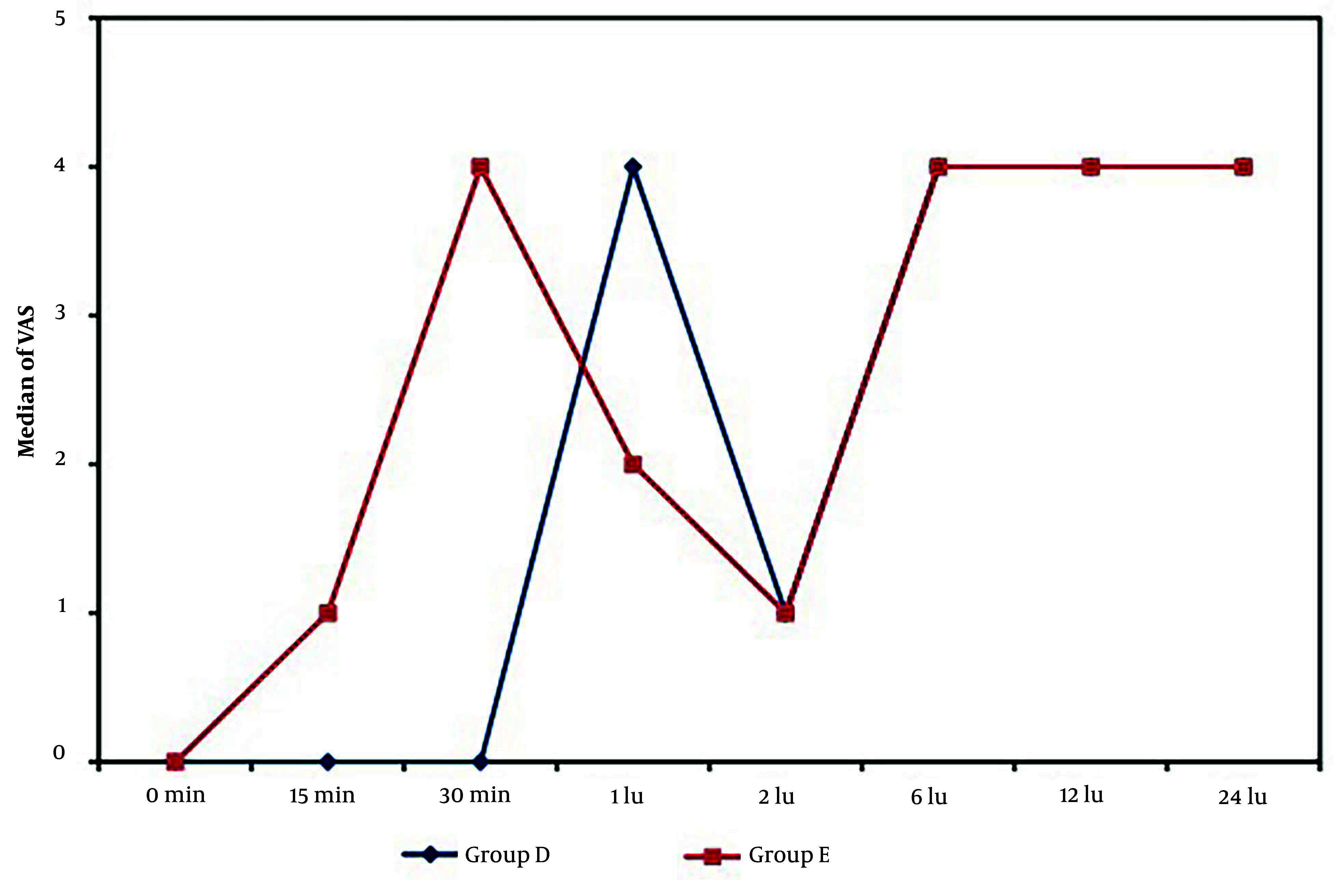
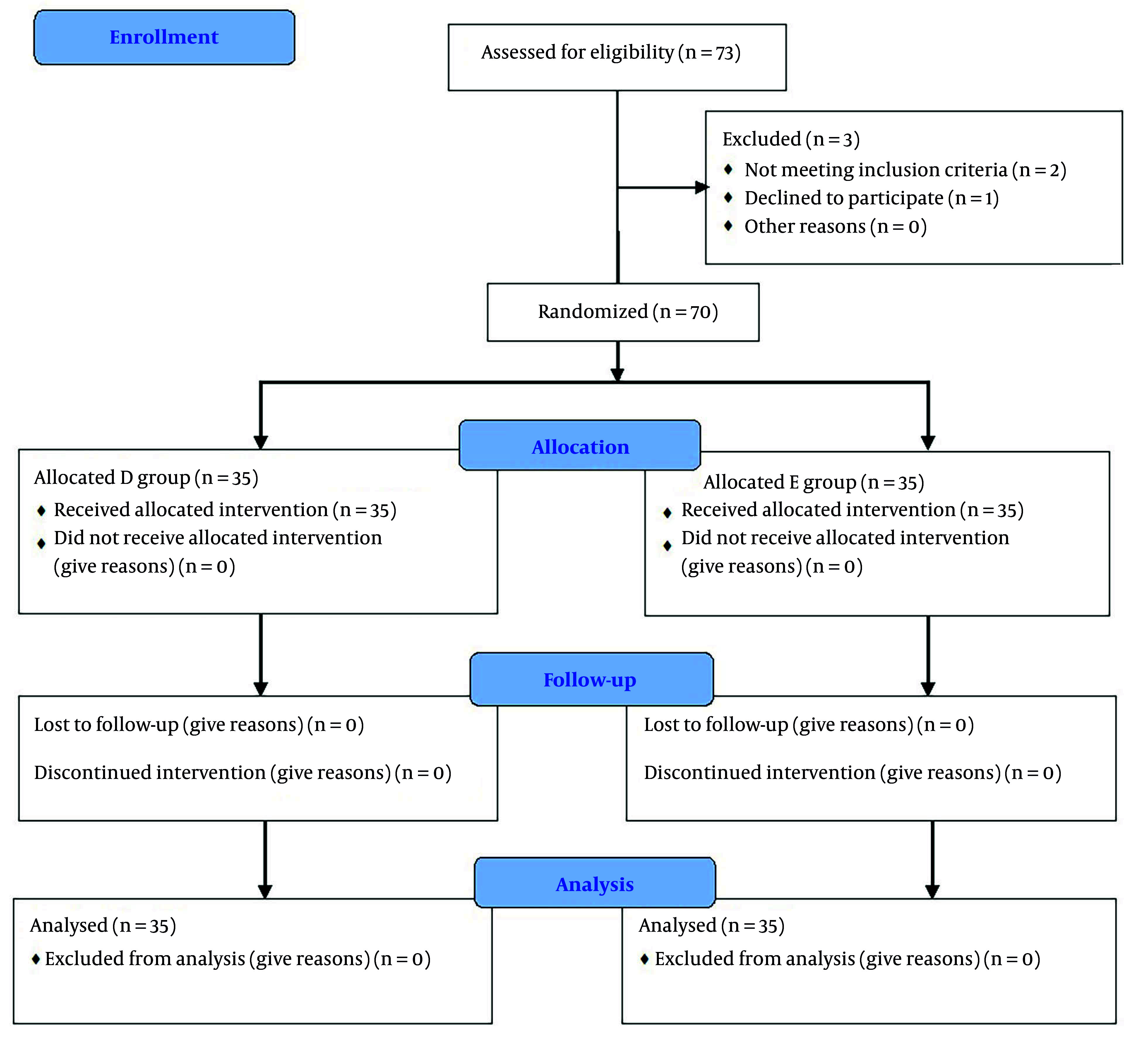
Methods: Seventy ASA I and II patients, of either sex, scheduled for FESS, were divided into two groups: The esmolol group (group E) received an intravenous bolus dose of 0.5 mg/kg prior to the induction of anesthesia, followed by 0.05 mg/kg/min and stopped immediately upon extubation, while the dexmedetomidine group (group D) received 1 µg/kg of dexmedetomidine over 10 minutes, immediately before the induction of anesthesia, followed by a 0.5 µg/kg/hour infusion after induction and stopped immediately upon extubation. Mean arterial pressure and heart rate were monitored before induction, before and after intubation, and then every 5 to 30 minutes, as well as every 10 minutes until 90 minutes following the commencement of the IV medication infusion. The sedation level was assessed using the Ramsay sedation scale at 15, 30, and 60 minutes postoperatively. Pain scores were evaluated in the recovery room (on arrival and then 15 minutes, 30 minutes, and 1 hour later) and at 2 hours, 6 hours, 12 hours, and 24 hours. The length of the procedure, the degree of bleeding during the intervention, and the occurrence of any adverse effects were documented. Categorical data were summarized as counts and percentages and compared by the chi-square test. Continuous data were assessed for normality using the Shapiro-Wilk test. The Student's t-test was used for quantitative variables that are normally distributed, whereas the Mann-Whitney test was used for quantitative variables that are not.
Results: According to our findings, both esmolol and dexmedetomidine were safe and beneficial in reducing blood loss during FESS, promoting optimal surgical field quality, and improving surgical field visibility. Dexmedetomidine was far more effective in providing postoperative sedation, reducing the need for opioids, and delaying the initial need for postoperative analgesia.
Conclusions: It was discovered that esmolol and dexmedetomidine both provided superior surgical field, less nasal hemorrhage, and more successful results. Dexmedetomidine caused effective sedation and a reduced need for analgesics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


