Polygenic risk scores for severe psychiatric disorders in bipolar disorders: associations with the clinical and dimensional expression, interactions with childhood maltreatment and mediation models.
Bruno Etain, Mohamed Lajnef, Ophélia Godin, Cynthia Marie-Claire, Frank Bellivier, Elisa Courtois, Violaine Latapie, Sébastien Gard, Raoul Belzeaux, Philippe Courtet, Caroline Dubertret, Emmanuel Haffen, Antoine Lefrere, Emilie Olie, Mircea Polosan, Paul Roux, Ludovic Samalin, Raymund Schwan, Marion Leboyer, Stéphane Jamain
{"title":"Polygenic risk scores for severe psychiatric disorders in bipolar disorders: associations with the clinical and dimensional expression, interactions with childhood maltreatment and mediation models.","authors":"Bruno Etain, Mohamed Lajnef, Ophélia Godin, Cynthia Marie-Claire, Frank Bellivier, Elisa Courtois, Violaine Latapie, Sébastien Gard, Raoul Belzeaux, Philippe Courtet, Caroline Dubertret, Emmanuel Haffen, Antoine Lefrere, Emilie Olie, Mircea Polosan, Paul Roux, Ludovic Samalin, Raymund Schwan, Marion Leboyer, Stéphane Jamain","doi":"10.1038/s41398-025-03466-5","DOIUrl":null,"url":null,"abstract":"<p><p>Polygenic risk scores (PRSs) for several psychiatric disorders have been associated with the clinical presentation of bipolar disorder (BD). PRSs have also been suggested to moderate the associations between childhood maltreatment and BD severity. In this study, we investigated how PRSs for BD, schizophrenia, major depressive disorders (MDD) and attention-deficit/hyperactivity disorder (ADHD) might disentangle the clinical and dimensional heterogeneity of BD in a sample of 852 affected individuals. We used logistic and linear regressions, moderation and mediation models to test the associations between PRSs, dimensions in childhood/adulthood and clinical indicators of severity of BD. All models were adjusted for age, sex, BD type and depressive symptoms. None of the PRSs were significantly associated with the clinical expression of BD when considered in terms of mode of onset, course, or psychiatric comorbidities. Nevertheless, the PRS-ADHD significantly and positively correlated with the levels of childhood maltreatment, childhood ADHD symptoms, and of some adulthood measures (affective lability, impulsivity and hostility) with p values ranging from 3.10<sup>-8</sup>-4.10<sup>-4</sup>. None of the PRSs moderated the effects of childhood maltreatment on the clinical or dimensional variables. Mediation model suggested paths from both PRS-ADHD and PRS-MDD to childhood ADHD symptoms and childhood maltreatment. The links between PRS-ADHD to all adulthood dimensions were mediated by childhood ADHD symptoms (p < 0.002). In turn, some adulthood dimensions (mainly affect intensity and affective lability) were associated with the clinical severity of BD, as defined by rapid cycling, suicide attempts and anxiety disorders. In conclusion, this study disentangles the associations between the genetic liability for four psychiatric disorders and the clinical/dimensional heterogeneity of BD. We suggest a continuum from the genetic risk for ADHD and MDD through dimensions in childhood/adulthood to a severe/complex clinical expression of BD.</p>","PeriodicalId":23278,"journal":{"name":"Translational Psychiatry","volume":"15 1","pages":"256"},"PeriodicalIF":6.2000,"publicationDate":"2025-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12297605/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational Psychiatry","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41398-025-03466-5","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
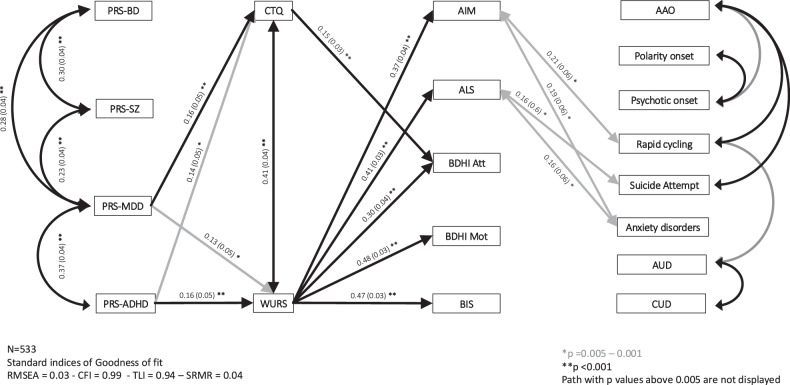
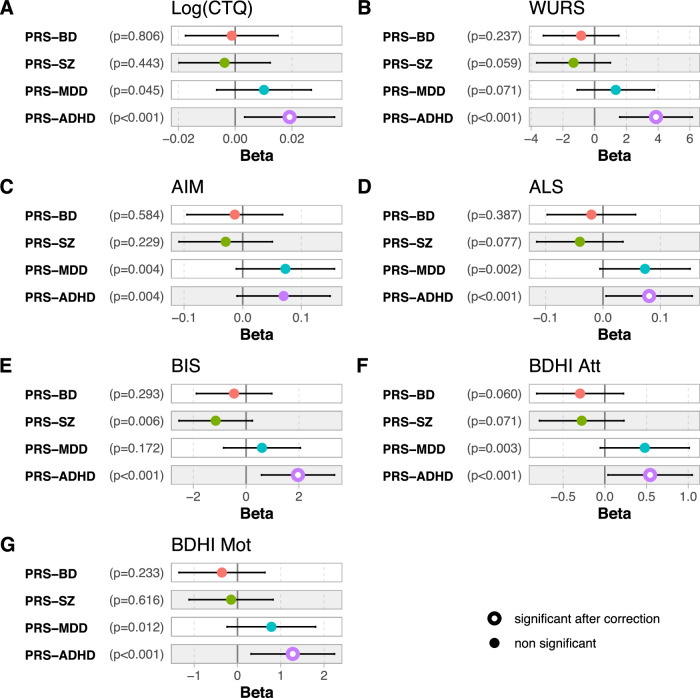
Polygenic risk scores (PRSs) for several psychiatric disorders have been associated with the clinical presentation of bipolar disorder (BD). PRSs have also been suggested to moderate the associations between childhood maltreatment and BD severity. In this study, we investigated how PRSs for BD, schizophrenia, major depressive disorders (MDD) and attention-deficit/hyperactivity disorder (ADHD) might disentangle the clinical and dimensional heterogeneity of BD in a sample of 852 affected individuals. We used logistic and linear regressions, moderation and mediation models to test the associations between PRSs, dimensions in childhood/adulthood and clinical indicators of severity of BD. All models were adjusted for age, sex, BD type and depressive symptoms. None of the PRSs were significantly associated with the clinical expression of BD when considered in terms of mode of onset, course, or psychiatric comorbidities. Nevertheless, the PRS-ADHD significantly and positively correlated with the levels of childhood maltreatment, childhood ADHD symptoms, and of some adulthood measures (affective lability, impulsivity and hostility) with p values ranging from 3.10-8-4.10-4. None of the PRSs moderated the effects of childhood maltreatment on the clinical or dimensional variables. Mediation model suggested paths from both PRS-ADHD and PRS-MDD to childhood ADHD symptoms and childhood maltreatment. The links between PRS-ADHD to all adulthood dimensions were mediated by childhood ADHD symptoms (p < 0.002). In turn, some adulthood dimensions (mainly affect intensity and affective lability) were associated with the clinical severity of BD, as defined by rapid cycling, suicide attempts and anxiety disorders. In conclusion, this study disentangles the associations between the genetic liability for four psychiatric disorders and the clinical/dimensional heterogeneity of BD. We suggest a continuum from the genetic risk for ADHD and MDD through dimensions in childhood/adulthood to a severe/complex clinical expression of BD.
期刊介绍:
Psychiatry has suffered tremendously by the limited translational pipeline. Nobel laureate Julius Axelrod''s discovery in 1961 of monoamine reuptake by pre-synaptic neurons still forms the basis of contemporary antidepressant treatment. There is a grievous gap between the explosion of knowledge in neuroscience and conceptually novel treatments for our patients. Translational Psychiatry bridges this gap by fostering and highlighting the pathway from discovery to clinical applications, healthcare and global health. We view translation broadly as the full spectrum of work that marks the pathway from discovery to global health, inclusive. The steps of translation that are within the scope of Translational Psychiatry include (i) fundamental discovery, (ii) bench to bedside, (iii) bedside to clinical applications (clinical trials), (iv) translation to policy and health care guidelines, (v) assessment of health policy and usage, and (vi) global health. All areas of medical research, including — but not restricted to — molecular biology, genetics, pharmacology, imaging and epidemiology are welcome as they contribute to enhance the field of translational psychiatry.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


