Alexandru Cristian Cindrea, Adina Maria Marza, Alexandra Maria Borita, Antonia Armega-Anghelescu, Ovidiu Alexandru Mederle
{"title":"Case Report: Spontaneous Pneumomediastinum and Pneumothorax Complicating Severe Ketoacidosis-An Unexpected Presentation.","authors":"Alexandru Cristian Cindrea, Adina Maria Marza, Alexandra Maria Borita, Antonia Armega-Anghelescu, Ovidiu Alexandru Mederle","doi":"10.3390/reports8020095","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background and Clinical Significance:</b> Diabetic ketoacidosis (DKA) is a serious and potentially life-threatening condition, often triggered by infections or undiagnosed diabetes. Spontaneous pneumomediastinum (SPM) and pneumothorax are rare but recognized complications of DKA, possibly due to alveolar rupture from increased respiratory effort or vomiting. Sometimes, acute pancreatitis (AP) may further complicate DKA, but the co-occurrence of these three conditions remains exceptionally rare. <b>Case Presentation:</b> We describe the case of a 60-year-old woman without a known history of diabetes who arrived at the emergency department with abdominal pain, fatigue, vomiting, and altered mental status. Initial laboratory findings showed metabolic acidosis, hyperglycemia, and elevated anion gap, consistent with DKA. Imaging revealed spontaneous pneumomediastinum and subsequently a left-sided pneumothorax, without evidence of trauma or esophageal rupture. Epigastric pain, along with elevated serum lipase and CT findings, also confirmed acute pancreatitis. Despite the complexity of her condition, the patient responded well to supportive treatment, including oxygen therapy, fluid resuscitation, insulin infusion, and antibiotics. She was discharged in good condition after 28 days, with a confirmed diagnosis of type 2 diabetes, without further complications. <b>Conclusions:</b> This case highlights an unusual combination of DKA complicated by spontaneous pneumomediastinum, pneumothorax and acute pancreatitis in a previously undiagnosed diabetic patient. Because prompt intervention can lead to favorable outcomes even in complex, multisystem cases, early recognition of atypical DKA complications is critical in order to avoid misdiagnosis.</p>","PeriodicalId":74664,"journal":{"name":"Reports (MDPI)","volume":"8 2","pages":""},"PeriodicalIF":0.8000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12197081/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reports (MDPI)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/reports8020095","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
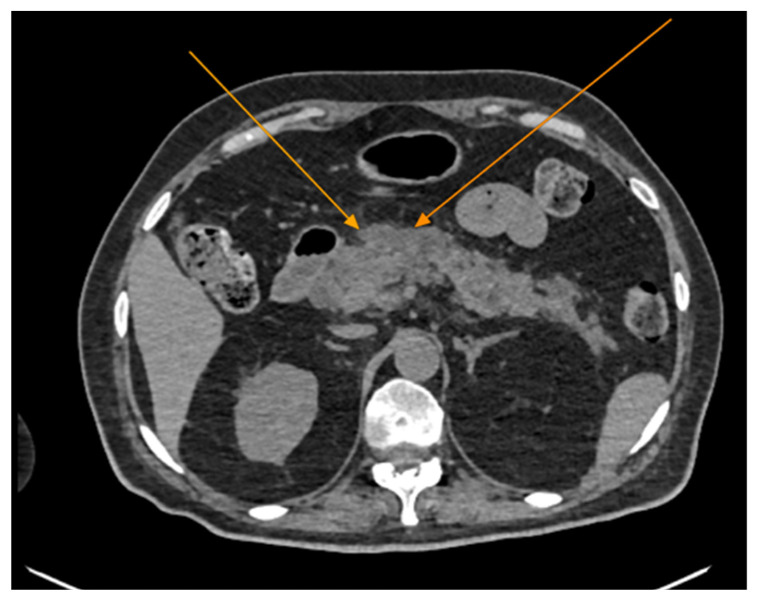
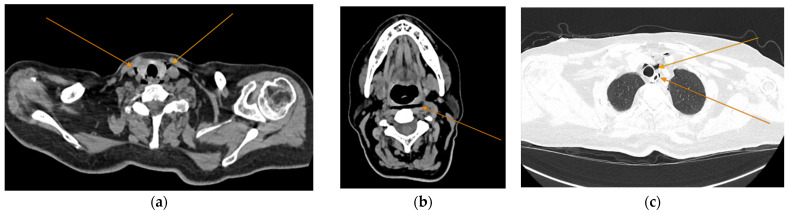
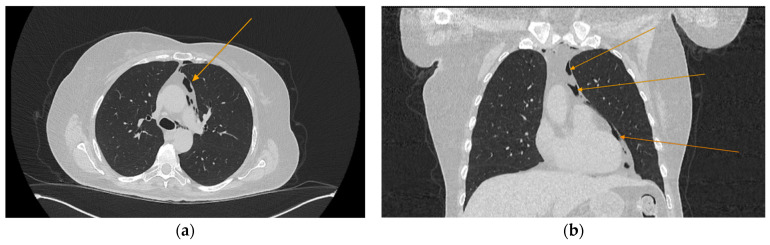
Background and Clinical Significance: Diabetic ketoacidosis (DKA) is a serious and potentially life-threatening condition, often triggered by infections or undiagnosed diabetes. Spontaneous pneumomediastinum (SPM) and pneumothorax are rare but recognized complications of DKA, possibly due to alveolar rupture from increased respiratory effort or vomiting. Sometimes, acute pancreatitis (AP) may further complicate DKA, but the co-occurrence of these three conditions remains exceptionally rare. Case Presentation: We describe the case of a 60-year-old woman without a known history of diabetes who arrived at the emergency department with abdominal pain, fatigue, vomiting, and altered mental status. Initial laboratory findings showed metabolic acidosis, hyperglycemia, and elevated anion gap, consistent with DKA. Imaging revealed spontaneous pneumomediastinum and subsequently a left-sided pneumothorax, without evidence of trauma or esophageal rupture. Epigastric pain, along with elevated serum lipase and CT findings, also confirmed acute pancreatitis. Despite the complexity of her condition, the patient responded well to supportive treatment, including oxygen therapy, fluid resuscitation, insulin infusion, and antibiotics. She was discharged in good condition after 28 days, with a confirmed diagnosis of type 2 diabetes, without further complications. Conclusions: This case highlights an unusual combination of DKA complicated by spontaneous pneumomediastinum, pneumothorax and acute pancreatitis in a previously undiagnosed diabetic patient. Because prompt intervention can lead to favorable outcomes even in complex, multisystem cases, early recognition of atypical DKA complications is critical in order to avoid misdiagnosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


