Marco Dominguez Davalos, Raúl Valenzuela Córdova, Celia Rodríguez Tudero, Elena Jiménez Mayor, Carlos Bedia Castillo, José C De La Flor, Roger Leon Montesinos, Cristian León Rabanal, Michael Cieza Terrones, Javier A Neyra
{"title":"An Unusual Case of Anuric Acute Kidney Injury Secondary to the Use of Low-Dose Acetazolamide as Preventive Management for Acute Mountain Sickness.","authors":"Marco Dominguez Davalos, Raúl Valenzuela Córdova, Celia Rodríguez Tudero, Elena Jiménez Mayor, Carlos Bedia Castillo, José C De La Flor, Roger Leon Montesinos, Cristian León Rabanal, Michael Cieza Terrones, Javier A Neyra","doi":"10.3390/diseases13070228","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background/Objectives</b>: Acetazolamide is widely used for acute mountain sickness (AMS) prophylaxis. Whilst generally safe, acute kidney injury (AKI) is a rare but serious adverse event. We present a case of anuric AKI following minimal exposure to acetazolamide, contributing to the limited literature on its nephrotoxicity at prophylactic doses. <b>Methods</b>: A 54-year-old previously healthy male ingested 250 mg/day of oral acetazolamide for two days. He developed acute anuria and lumbar pain. Diagnostic evaluation included laboratory tests, imaging, microbiological cultures, autoimmune panels, and diuretic response. No signs of infection, urinary tract obstruction, or systemic disease were found. <b>Results</b>: The patient met KDIGO 2012 criteria for stage 3 AKI, with peak serum creatinine of 10.6 mg/dL and metabolic acidosis. Imaging confirmed non-obstructive nephrolithiasis. Conservative treatment failed; intermittent hemodialysis was initiated. Renal function recovered rapidly, with the normalization of serum creatinine and urinary output by day 4. <b>Conclusions</b>: This case represents the lowest cumulative dose of acetazolamide reported to cause stage 3 AKI. The findings support a pathophysiological mechanism involving sulfonamide-induced crystalluria and intratubular obstruction. Physicians should consider acetazolamide in the differential diagnosis of AKI, even with short-term prophylactic use.</p>","PeriodicalId":72832,"journal":{"name":"Diseases (Basel, Switzerland)","volume":"13 7","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2025-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12293891/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diseases (Basel, Switzerland)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/diseases13070228","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
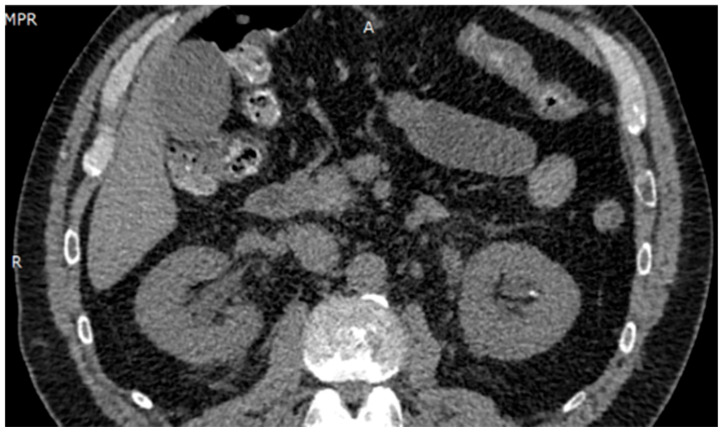
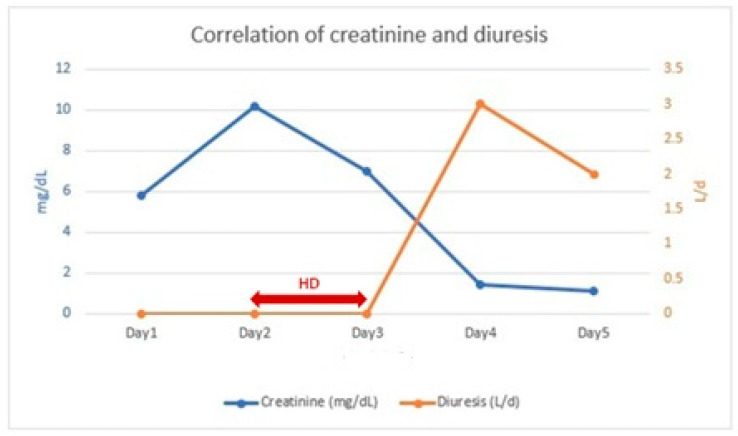
Background/Objectives: Acetazolamide is widely used for acute mountain sickness (AMS) prophylaxis. Whilst generally safe, acute kidney injury (AKI) is a rare but serious adverse event. We present a case of anuric AKI following minimal exposure to acetazolamide, contributing to the limited literature on its nephrotoxicity at prophylactic doses. Methods: A 54-year-old previously healthy male ingested 250 mg/day of oral acetazolamide for two days. He developed acute anuria and lumbar pain. Diagnostic evaluation included laboratory tests, imaging, microbiological cultures, autoimmune panels, and diuretic response. No signs of infection, urinary tract obstruction, or systemic disease were found. Results: The patient met KDIGO 2012 criteria for stage 3 AKI, with peak serum creatinine of 10.6 mg/dL and metabolic acidosis. Imaging confirmed non-obstructive nephrolithiasis. Conservative treatment failed; intermittent hemodialysis was initiated. Renal function recovered rapidly, with the normalization of serum creatinine and urinary output by day 4. Conclusions: This case represents the lowest cumulative dose of acetazolamide reported to cause stage 3 AKI. The findings support a pathophysiological mechanism involving sulfonamide-induced crystalluria and intratubular obstruction. Physicians should consider acetazolamide in the differential diagnosis of AKI, even with short-term prophylactic use.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


