Krithika Sundaram, Veenah Stoll, Luciana Da Fonseca Da Silva, Adam Christopher, Arvind Hoskoppal, Jacqueline Kreutzer, David Liddle, Laura Olivieri, Jacqueline Weinberg, Craig P Dobson, José P Da Silva, Tarek Alsaied
{"title":"Mid-Term Recovery of Right Ventricular Function and Improvement of Left Ventricular Function After Da Silva Cone Procedure for Ebstein Anomaly.","authors":"Krithika Sundaram, Veenah Stoll, Luciana Da Fonseca Da Silva, Adam Christopher, Arvind Hoskoppal, Jacqueline Kreutzer, David Liddle, Laura Olivieri, Jacqueline Weinberg, Craig P Dobson, José P Da Silva, Tarek Alsaied","doi":"10.3390/jcdd12070276","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Da Silva Cone procedure for Ebstein anomaly has dramatically improved tricuspid valve competence and clinical outcomes. However, preoperative left ventricular (LV) dysfunction and immediate postoperative right ventricular (RV) systolic dysfunction are frequently observed. While excellent valve outcomes are well established, recovery of biventricular function following the Cone remains less defined. This study aimed to evaluate longitudinal changes in RV and LV function postoperatively and over a minimum of six months post-Cone operation.</p><p><strong>Methods: </strong>A single center retrospective review of 134 patients who underwent Cone repair for Ebstein's anomaly from 2016 to 2024 was performed. Echocardiograms were analyzed at three time points: preoperative (Time 1), hospital discharge (Time 2), and ≥6 months postoperative (Time 3). RV parameters included fractional area change (FAC), tricuspid annular plane systolic excursion (TAPSE), and tricuspid S'. LV parameters included left ventricular ejection fraction (LVEF), end-diastolic volume indexed to body surface area (LVEDVi), left ventricular stroke volume (LVSVi), and mitral E/E'. Subgroup analyses examined outcomes by prior Glenn, Starnes procedure, and degree of RV dilation. Paired two sample <i>t</i>-tests were used to compare serial measures.</p><p><strong>Results: </strong>Median age at surgery was 7.8 years (IQR: 2.3-17.7). All patients had discharge echocardiograms; 70 had follow-up studies at ≥6 months. RV function declined postoperatively with reductions in FAC (35% to 21%), TAPSE (2.0 to 0.8 cm), and S' (13 to 5 cm/s), all <i>p</i> < 0.001. By Time 3, these measures improved (FAC to 29%, TAPSE to 1.3 cm, S' to 7 cm/s) but did not fully return to baseline. LVEDVi and LVSVi increased significantly by Time 3 (LVEDVi: 47 to 54 mL/m<sup>2</sup>; LVSVi: 30 to 34 mL/m<sup>2</sup>; <i>p</i> < 0.001), while LVEF remained unchanged. Patients with prior Glenn or Starnes had greater Time 1 LV volumes and lower RV function, but by Time 3, most differences resolved. Moderate-severe preoperative RV dilation was associated with worse RV function at Time 2 and normalized by Time 3.</p><p><strong>Conclusions: </strong>The Da Silva Cone procedure leads to early postoperative RV dysfunction with partial recovery over the mid-term follow-up. Concurrently, LV filling and stroke volume improve, reflecting favorable interventricular interaction. These findings support echocardiographic surveillance to guide functional recovery post-Cone and inform patient counseling.</p>","PeriodicalId":15197,"journal":{"name":"Journal of Cardiovascular Development and Disease","volume":"12 7","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12295748/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Development and Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/jcdd12070276","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The Da Silva Cone procedure for Ebstein anomaly has dramatically improved tricuspid valve competence and clinical outcomes. However, preoperative left ventricular (LV) dysfunction and immediate postoperative right ventricular (RV) systolic dysfunction are frequently observed. While excellent valve outcomes are well established, recovery of biventricular function following the Cone remains less defined. This study aimed to evaluate longitudinal changes in RV and LV function postoperatively and over a minimum of six months post-Cone operation.
Methods: A single center retrospective review of 134 patients who underwent Cone repair for Ebstein's anomaly from 2016 to 2024 was performed. Echocardiograms were analyzed at three time points: preoperative (Time 1), hospital discharge (Time 2), and ≥6 months postoperative (Time 3). RV parameters included fractional area change (FAC), tricuspid annular plane systolic excursion (TAPSE), and tricuspid S'. LV parameters included left ventricular ejection fraction (LVEF), end-diastolic volume indexed to body surface area (LVEDVi), left ventricular stroke volume (LVSVi), and mitral E/E'. Subgroup analyses examined outcomes by prior Glenn, Starnes procedure, and degree of RV dilation. Paired two sample t-tests were used to compare serial measures.
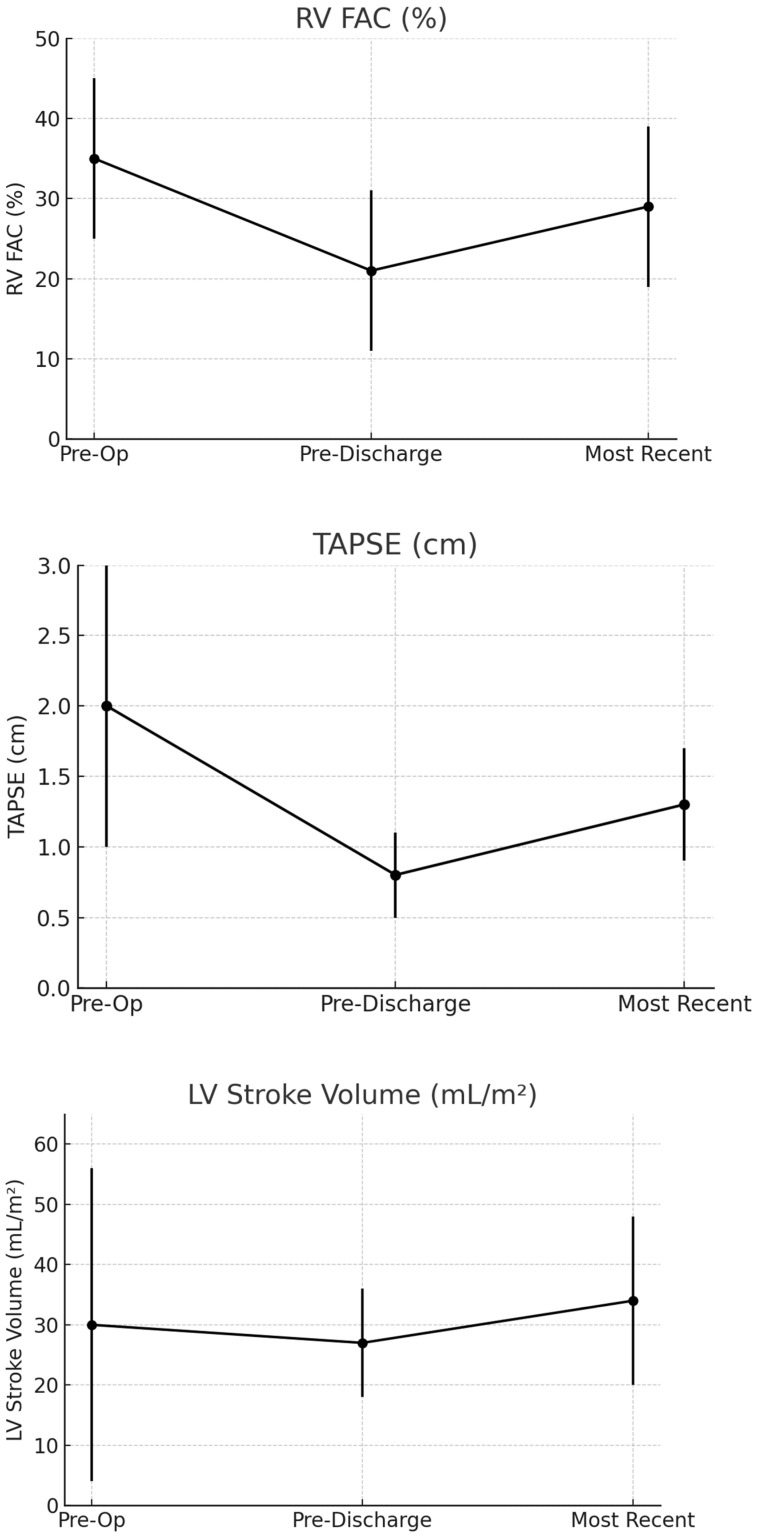
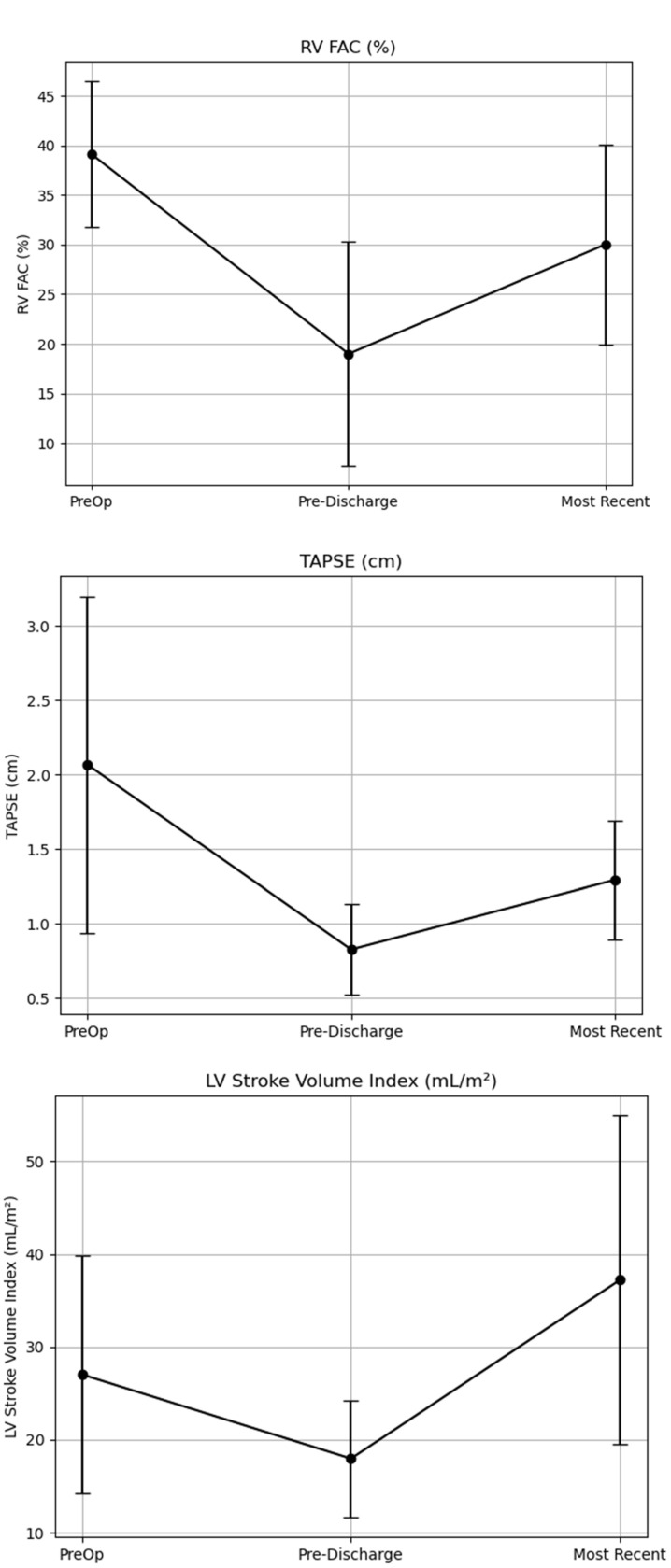
Results: Median age at surgery was 7.8 years (IQR: 2.3-17.7). All patients had discharge echocardiograms; 70 had follow-up studies at ≥6 months. RV function declined postoperatively with reductions in FAC (35% to 21%), TAPSE (2.0 to 0.8 cm), and S' (13 to 5 cm/s), all p < 0.001. By Time 3, these measures improved (FAC to 29%, TAPSE to 1.3 cm, S' to 7 cm/s) but did not fully return to baseline. LVEDVi and LVSVi increased significantly by Time 3 (LVEDVi: 47 to 54 mL/m2; LVSVi: 30 to 34 mL/m2; p < 0.001), while LVEF remained unchanged. Patients with prior Glenn or Starnes had greater Time 1 LV volumes and lower RV function, but by Time 3, most differences resolved. Moderate-severe preoperative RV dilation was associated with worse RV function at Time 2 and normalized by Time 3.
Conclusions: The Da Silva Cone procedure leads to early postoperative RV dysfunction with partial recovery over the mid-term follow-up. Concurrently, LV filling and stroke volume improve, reflecting favorable interventricular interaction. These findings support echocardiographic surveillance to guide functional recovery post-Cone and inform patient counseling.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


